
Patho Micro Made Easy
Dr K Chaudhry
FIRST Author of Jaypee Brothers
Content
|
|
Page |
|
|
01 |
Clinical Pathology |
3 |
|
02 |
Haematology |
58 |
|
03 |
Inflammation and Repair |
93 |
|
04 |
Circulatory Disturbances |
127 |
|
05 |
Nutritional Disturbances |
141 |
|
06 |
Granulomata |
170 |
|
07 |
Tumours |
177 |
|
08 |
Cardiovascular System |
185 |
|
09 |
Urinary System |
205 |
|
10 |
Respiratory System |
226 |
|
11 |
Alimentary System |
247 |
|
12 |
Miscellaneous Topics |
267 |
|
13 |
General Bacteriology |
277 |
|
14 |
Systematic Bacteriology |
295 |
|
15 |
Virology |
350 |
|
16 |
Parasitology |
366 |
|
Chapter 1 : Clinical Pathology BLOOD EXAMINATION Bleeding Time Duke's method: Prick the ear lobe or palmar surface of a finger tip sufficiently to induce a free flow of blood. It should be practised to produce a blot of 1-2 cms at the end of a minute. At the end of every half a minute blot with a piece of filter paper, making a row of blots, till the blood flow ceases. Bleeding time in minutes is number of blots divided by two. The normal bleeding time is 1-3 minutes. It is enhanced in platelet deficiency and fibrinogen deficiency, but not in hemophilia.
Bleeding & coagulation time : Duke method Coagulation Time 1. With capillary blood: A wound is pricked as above and the blood is flown into a capillary tube, about 1.5 mm in diameter. Short sections of tube are then broken off every minute until fibrin thread appears between the broken ends. The coagulation time is the interval between the start of blood flow and the last break point. The normal coagulation time with this method is 3-5 minutes 2. With Venous Blood (i) Lee & White method: This can be combined with serum separation for biochemistry and immunological tests. Blood is drawn through a hypodermic needle into an 8 mm diameter glass tube. It is tilted every minute till it can be inverted without displacing the clot. Time is counted from the point at which blood starts flowing out of the needle. The normal coagulation time with this method is 5-10 minutes. It increases with tube diameter. (ii) Howell's method: It is similar to Lee & White method except the treatment of syringe before use. Fill the syringe alongwith needle with ether-petrolatum mixture. Force the mixture out and draw air into the syringe a few times. Ether will evaporate leaving petrolatum coating. Draw 2-4 ml blood into the syringe and empty it into glass tube about 2 cms in diameter. Proceed as in preceding method. Normal coagulation time with this method is 10-30 minutes. Prothrombin Time Quick's method: Mix 0.4 ml sodium oxalate 0.1 M with 1.6 ml fresh blood. Invert 2-3 times to mix thoroughly. Centrifuge to obtain clear plasma. Mix 0.1 ml plasma with 0.1 ml thromboplastin suspension. Incubate at 37ºC
for about 5 minutes. Add quickly 0.1 ml calcium chloride M/14 solution and
start the stop-watch. The end point is one at which the tube can be tilted to
horizontal position without displacing the clot.
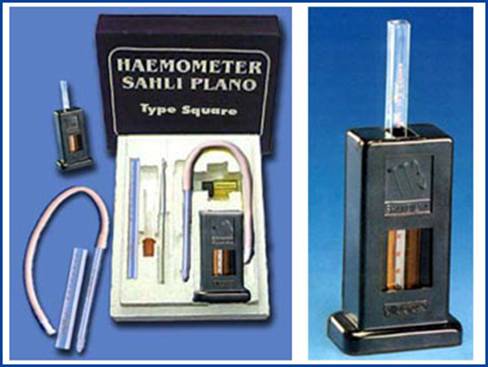
Prothrombin time chart Haemoglobin Haemoglobin may be estimated as acid hematin, oxyhemoglobin or cynmethemoglobin. Acid hematin method with Sahli's hemoglobinometer is most suitable for bed side diagnosis. Cynmethemoglobin method is most widely used with colorimeter. However, both the reagent and the standard are poorly stable. The acceptable proposal for cynmethemoglobin method would be to use manufacturer's standard first week and to use carboxyhemoglobin (final solution) prepared from first sample of every week, as a standard during the week. Thus a chain of fresh standards may work for the kit life. Sahli's method
Place hydrochloric acid N/10 in hemometer tube upto mark 10. Pour into it, 0.02 ml fresh or oxalated whole blood from Sahli's pipette. Mix with the glass rod. Place the tube in the frame. After a minute, dilute the mixture with water drop by drop, mixing after each addition, until the colour shade matches exactly with the standard shade on the frame. The reading corresponding to the surface of final solution gives hemoglobin concentration in the blood, both as g% and as percentage of normal. Haemocytometer
Hemocytometer comprises a thick counting slide (Neubauer counting slide) with two pipettes, and is used for erythrocyte and leucocyte counting. Erythrocyie pipette, with red identification bead bears three marks 0.5, 1 and 101. Presuming the capillary part upto mark 1 as unmixed with blood, the pipette is used to dilute the blood 1:100 or 1:200 with erythrocyte diluting fluid. Leucocyte pipette, with white identification bead bears 0.5, 1 and 11 marks. This can be used for 1:10 and 1:20 dilutions of blood with leucocyte diluting fluid. The dilution can be more conveniently made with ordinary pipettes. Neubauer counting slide has two counting areas, for two samples at a time with a separating groove. The counting areas, each comprising 9 large squares of 1 square mm area are slightly depressed. A specially ground coverslip placed over the counting area gives a depth of 0.1 mm. Thus each one of the 9 large squares covered with the coverslip holds a volume of 0.1 cu.mm. Total erythrocyte count
The fluids develop molds with time and have to be filtered frequently. The author overcame this problem by using benzoic acid 0.1% in place of distilled water. Total leucocyte count Turk's leucocyte diluting fluid is prepared as follows: Acetic acid glacial 1 ml
This fluid develops moulds and has to be filtered frequently. Moulds can be prevented by using benzoic acid 0.1% in place of distilled water.
Central large square of Neubauer
counting slide, intended for erythrocyte counting, is divided into
25 sets of 16 small squares each. Erythrocytes in four corner sets and the
central set are counted. The volume of the counted space is 0.02 cu mm.
Erythrocyte Counting 1.
Suck up the
capillary blood from finger tip or car lobe to the mark 0.5.
The erythrocytes lying over upper and left edges of small square should be counted; those or right and lower edges should be ignored. Calculation
1 = C x 10,000 per cu. mm Where C is the count in 5 x 16 squares, 0.02 the volume of counted space and 200 the dilution factor. Leucocyte Counting Proceed as with
erythrocyte counting, using Turk's fluid. Take blood to mark 0.5 and dilute
to mark 11.
Count the leucocytes in four large squares at the corners and divide with 4 to get the average. Calculation
1 = C x 200 per cu. mm. where C is the average
count in one large square (16 small squares), 0.1 the volume covered and 20
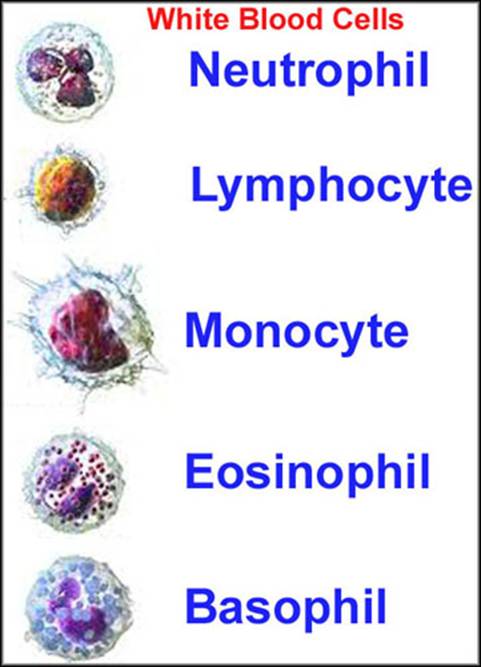
the dilution used. Differential leucocyte count Differential leucocyte counting is done on a stained peripheral blood smear. The slides used should be cleaned and defatted. Used slides should be cleaned by boiling in sodium carbonate 1% solution. The slides should then be rinsed with distilled water, kept under a stream of running water for a few hours and finally stored in ethanol-ether mixture (1 + 1). Before using, the slides should be dried and then wiped with linen cloth. In order to prepare a blood smear, touch the slide surface with the blood welling up from the finger tip or ear lobe. Take a clean polished coverslip (square shape), hold it between thumb and index finger, and press its edge gently over the droplet until the droplet runs along the edge. Then holding the coverslip at an angle of 45º, spread the blood with a motion to give a uniform even smear. Make two or three smears and stain one at a time. Leishman Staining The staining solution is prepared by dissolving 1.5g powdered stain in a litre of methanol. The solution should be shaken vigorously during the first 24 hours. The blood smear is covered with 10 drops of Leishman stain for 30-60 seconds, making sure that the smear remains wet. More stain may be poured, if necessary. 20 drops of distilled water are then poured over the stain. The slide is rocked gently in order to mix the stain well with distilled water. After 10 minutes, the smear is rinsed with running tap water, dried in air, and examined under oil immersion lens. Types of Leucocytes At least one hundred
leucocytes should be differentiated into neutrophils (polymorphonuclears),
lymphocytes, monocytes, eosinophils, basophils and abnormal cells.
Thrombocyte Counting Any of the following solutions may be used as platelet diluting fluid. 1. Ammonium oxalate 1%. 2. Sodium citrate
3.8% 100 ml 3. Sodium
oxalate 1.6 g
The first solution is preferred by experienced technicians whereas the latter 2 solutions are more suitable for freshers. The blood is diluted 1:10 with diluting fluid with the help of leucocyte pipette. Further procedure is same as for erythrocyte counting. Multiplication factor is 1,000 in place of 10,000. URINE EXAMINATION Collection of Specimen A. For routine examination. Spontaneous urine sample should be collected in a clean jar. Time of passing urine sample should be such that urine is most likely to contain the pathological constituent being sought viz. 1. Inflammatory
disease. Morning sample. Only fresh urine should be used to study the urinary sediments. B. For bacteriological examination. Preferably a morning specimen should be collected in a clean sterile flask. A catheter specimen is essential in female patients and desirable in male patients. In males, an inferior alternative is mid-stream urine. Glans penis and urethral meatus are cleaned with several swabs soaked in normal saline. The first portion of urine is discarded and mid-stream sample is collected in a sterile flask. The last portion is also discarded. C. For chorionic gonadotrophin test. For UCG pregnancy test, a morning specimen is desirable. Patient should not take water in the morning till specimen is collected. Drugs such as salicylates, barbiturates should not be taken for at least two days prior to collection. D. For quantitative estimations. A 24 hour collection of urine should be pooled in a sterile (or hot water washed) glass vessel. At the beginning of the stipulated 24 hour period, the bladder must be emptied and the urine collected discarded. At the end of 24 hour period, the hladder should again be emptied and urine included in the pool; 5 mI of 10% thymol should be added to preserve 24 hour pool. Alternatively 3-4 drops of toluene should be added to form a thin film on the surface. General tests Urine output. 24 hour urine output varies with: (i) Fluid intake Nonnal Values
The day
time output is 2-4 times the night time output. The reverse (nycturia) is an
early sign of. Oliguria. Urine output less than 500 ml/24 hours. Observed in:
Polyuria. Urine output more than 2500 ml/24 hours. Observed in:
Urine Colour
Urine turbidity. Normal urine, when passed is clear. On standing for some time, a flocculent sediment (nubecula) settles down. Turbidity of urine can be assessed with the following scheme. Heat a few ml of urine in
a water bath or over a flame
Specific gravity. The specific gravity is conventionally measured as milligrams per cubic centimetre. Thus a specific gravity of 1.015 is written as 1015. It is measured with a urinometer having callibrations of 1000-1040. The urinometer is made to float in a glass container (flask or wide tube) so that it does not touch the bottom or sides of the container. The normal value is 1015-1025. Sugar and protein increase the density of urine. To make specific gravity an index of renal function, the following allowances should be made., 1. Add 0001 for every 3ºC above callibration temperature (usually 15ºC) of the urinometer. Subtract 0001 for every 3ºC below the callibration temperature. 2. Subtract 0003.7 for every 1% glucose and 0002.6 for every 1 % protein. Reaction. Normal urine is acidic (pH 4.8 - 7.4). Strongly acidic in: (i) Malignancy (ii) Fever (iii) Severe diarrhoea (iv) Diabetic and metabolic acidosis. Alkaline in: (i) Urinary infections
Chemical Tests
1. Protein Normally the urine contains very little amount of proteins with low molecular weight. In pathological conditions, the permeability of glomeruli changes thus increasing the protein content of urine, mainly of serum albumin. The proteins excreted in urine may be of following types:
Detection of proteins may be made with the following tests 1 Purdy's heat test. Check the reaction of urine and if alkaline, add 10% acetic acid drop by drop until the litmus paper shows just acidic reaction. Incline at an angle and boil the top 2 cm over a flame, holding the bottom of the test tube. Examine against a dark background. A cloudy appearance indicates protein or phosphates. Add a few drops of 10% acetic acid and boil again. If cloud disappears, it indicates phosphates; a persistent cloud indicates protein. False positive results may be observed in patients receiving tolbutamide, high doses of penicillin or radiographic contrast media. 2. Robert's test. Place 2-3 ml Robert's reagent in a test tube and gently layer a few drops of urine over it. Albumin gives a white ring which varies in density with the amount of albumin present. 3. Heller's test. The procedure is the same as for Robert's test. Concentrated nitric acid is used in place of Robert's reagent. 4. Sulphosalicylic acid test. Take 5 ml urine in a test tube. Add 0.5 ml sulphosalicylic acid 20%. Albumin gives white precipitate.
Esbach’s Albuminometer Quantitative test for protein Fill up the albuminometer to mark U with urine. Add Esbach's reagent to mark R. Close the tube with a rubber stopper, invert it slowly several times, and set it aside in a cold place. At the end of 24 hours read the height of the precipitate in grams/ litre. Divide it with 10 to get percentage. Causes of Proteinuria
Bence-Jones Proteins Bence-Jones proteins are paraproteins rich in carbohydrates and lipids. These are present in patients with:
These proteins produce milky turbidity at 45oC, which clears on further heating to 60oC. 2. Sugar. Normal urine contains minute quantity of glucose not detected by ordinary tests. A detectable concentration of glucose in urine is termed glycosuria. The usually employed method of detection is Benedict's test. Benedict's test. To 5 ml of Benedict's qualitative reagent add 8 drops of urine. Boil for 2 minutes and allow to cool. Note the change in colour or precipitate formation. The result may be interpreted as under:
False positive results maybe given by the presence of reducing agents, e.g., uric acid, creatinine, ascorbic acid, glucuronic acid, penicillin, tetracycline, paraaminosalicylic acid, salicylates. Causes of Glycosuria
3. Acetone bodies. Presence of acetone bodies such as acetone, diacetic (acetoacetic) acid and betaoxybutyric acid is always abnormal. It occurs in diabetes mellitus and starvation due to neoglucogenesis after glycogen stores in the liver have been depleted Tests for Acetone (i) Rothera's test. Place about 5 ml urine in a test tube and add about 1 g ammonium sulphate followed by 2-3 drops of concentrated sodium nitroprusside solution. Add 1 ml concentrated ammonium hydroxide solution. A permanganate coloured ring indicates the presence of acetone. (ii) Lange's test. As above but adding 5 drops of glacial acetic acid in place of ammonium sulphate. (iii) Frommer's test. Add 2-3 ml sodium hydroxide 10 N to 10 ml urine. Add 10-12 drops of 10% salicylaidehyde (alcoholic). Heat the upper portion to about 700C without reaching boiling point for at least 5 minutes. A yellow, orange, red or brown colour indicates acetone. Tests for Diacetic Acid
The test should be confirmud, if positive, on urine diluted with equal volume of water and boiled off to original volume. Colour due to diacetic acid will not appear in confirmatory test. Colour in confirmatory test is due to other substances such as phenol ' salicylates, antipyrine and sodium bicarbonate. Lindematin's test should be performed in such cases. 2. Lindemann's test. To 10 in] urine, add 5 drops of 30% acetic acid and 5 drops of 5% iodine solution (in 10% potassium iodide). Then add 2-3 drops of chloroform. In the presence of diacetic acid, chloroform will not become reddish violet. Tests for
Beta-oxybutytic Acid 4. Bile salts.
False positive results may be given by high concentrations of urobilin or if thymol is used as preservative. Causes (i) Obstructive jaundice.
5. Bile pigment.
(b) Gmefin's test. Take 3 ml of concentrated nitric acid in a test tube. Add an equal amount of urine. A green or blue ring indicates bilirubin. 6. Urobilin
(urobilinogen) 7. Blood. Benzidine
test. Dissolve a pinch of benzidine in glacial acetic acid. Add 2 ml of
urine, previously boiled and cooled, to 1 ml benzidine solution. Mix and add
1 ml of 3% hydrogen peroxide. Wait for 5 minutes. A green or blue colour
Causes of Haematuria
8. Hemosiderin 9. Porphobilinogen 10. melanin 11. Diazo substances Prepare diazo reagent by mixing 10 ml 0.5% sulphanilic acid solution with 0.1 ml 0.5% sodium nitrite solution. Mix 5 ml -each of urine and diazo reagent by inversidn. Add 1-2 ml liquid ammonia. If the reaction is positive, garnet ring will appear at the junction and on shaking the foam will be coloured deep red. Yellow or orange colour should be ignored. The reaction becomes positive on 4-5th day of typhoid fever and fades during third week. An early fading is a favourable sign. It may also be positive in pulmonary tuberculosis and measles. Microscopic Examination A sample of urine is centrifuged at 1000-1500 rpm for about 3 minutes. The upper clear portion is discarded as much as possible and the centrifuge tube is then shaken to form homogenous suspension of the sediment. A drop is placed on the slide and covered with a cover slip. The slide is examined under high power objective of the microscope and a search is made for the following: 1. Erythrocytes. Normal urine shows upto one erythrocyte per high power field. Excess blood in urine is termed haematuria. Causes of hematuria are enumerated above in this chapter. 2. Leucocytes. A few leucocytes or pus cells are present in normal urine. Upto 5 cells per high power field may be considered as normal. Abnormal amount of leucocytes in urine is seen in inflammatory conditions of the urinary tract, renal tuberculosis and following catheterisation. 3. Casts. Hyaline casts result from precipitation of mucoprotein in the renal tubules. On hyaline casts materials such as erythrocytes, leucocytes, epithelial cells may be deposited. On microscopic examination casts are recognised as cylinderical bodies with sharply defined outline and rounded ends one of which may be 'broken'. Casts of following types may be detected:
4. Crystals (a) In acid urine: (i) Calcium oxalate (ii) Uric acid (iii) Urates. (b) In Alkaline urine: (i) Amorphous phosphates (ii) Ammonium urate. STOOL EXAMINATION Gross Examination
1. Colour
2. Odour
3. Mucus
4. Pus. (with blood and
mucus) 5. Concretions. Gallstones. 6. pH. Normal pH is 6.8 - 7.3. Excess of carbohydrate produces acidity and excess of protein alkalinity. 7. Occult blood (i) Benzidine test. Already described. (ii) Orthotoluidine test. Prepare thick suspension of feces. Add 1 mJ, of orthotoluidine reagent and 1 mI of 3% hydrogen peroxide. Observe for a minute. Bluish green colour indicates occult blood. Microscopic Examination Transfer one drop of thick stool suspension (in normal saline) onto a slide. Cover with coverslip and examine first under low power objective and then under high power objective. One more slide should be prepared and examined in the same way adding a drop of weak iodine solution. Concentration Methods 1. De Riva's inethod. Place about 1 g stool in a test tube. Add 5 ml 5% acetic acid. Close the tube and shake vigorously for half a minute. Keep still for half a minute coarse particles will sink rapidly to the bottom. Pipette out homogeneous supernatant into a centrifuge tube. Add an equal volume of ether. Close the tube and shake vigorously for half a minute. Centrifuge for 5 minutes. The contents will differentiate into four layers: (i) Ethereal layer (for
occult blood) Findings Cysts of protozoa viz.
Cyst of Entamoeba histolytica (ii) Entamoeba coli
Cyst of Entamoeba coli (iii) Giardia intestinalis
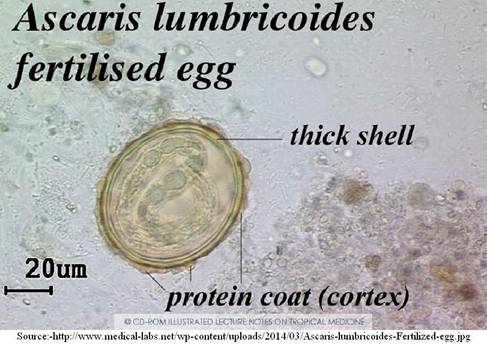
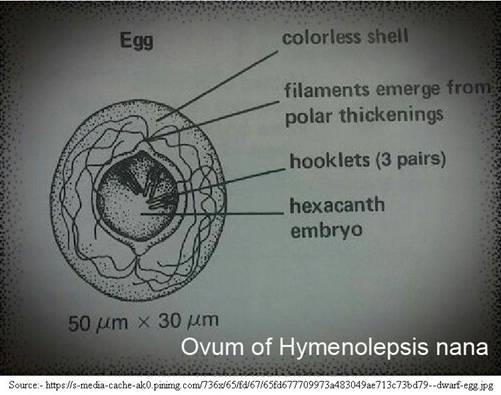
Ova of helminths viz.
(ii) Enterobius vermicularis
SPUTUM EXAMINATION
B. Microscopic Examination (unstained) 1. Elastic fibres (ii) Lung abscess (iii) Gangrene. 2. Curschmann’s spirals - Bronchial asthma 3. Charcot-Leydon crystals- Bronchial asthma 4. Pigmented cells
5. Myeline globules - No significance 6. Molds, yeasts and parasites. C. Microscopic Examination (stained) Several smears should be stained with AJFB stain, Gram stain and for capsules. 1. AFB Staining a. Hot method. Cover the smear with carbol fuchsin (strong). Heat it over flame till it steams for 3 minutes. Stain should not dry out; add more staining solution as necessary. Rinse with water and pour sulphuric acid 20% or, preferably, hydrochloric acid 3% in ethanol till pink stain ceases to flow out. Rinse with water and counterstain with Loffier's methylene blue for two minutes. b. Cold method. The smear slide is air dried on a warming plate. The slide
is prefixed in a Coplin jar of absolute methanol for 5 to 10 s, stained in
carbol fuchsin-DMSO solution in a Coplin jar for 5 min, and rinsed
individually in gently running tap water until excess solution no longer ran off
(10 to 30 s per slide). Slide is then placed in the decolorizer-counterstain
for 1 min or until a green background appeared and then is rinsed under
running tap water for 10 s, drained, blotted, and placed on a warming plate
until thoroughly dry (5 or 10 min). A thin film of immersion oil is applied
over smear with an applicator stick. For the carbol fuchsin-DMSO stain, 4 g of basic fuchsin crystals is dissolved in 25 ml of 99% ethyl alcohol. 12 grams of phenol crystals liquefied in a water bath (or 12 ml of liquefied phenol) is added and mixed well with a glass stirring rod. Then, 25 ml of glycerol, chemically pure, 25 ml of DMSO and 75 ml of distilled water are added and mixed well. The solution is allowed to stand for 30 min and then filtered, The stain may be used immediately or kept indefinitely at room temperature in an amber glass bottle. For the decolorizer-counterstain solution, 220 ml of a 2% aqueous solution of malachite green is prepared; 30 ml of glacial acetic acid (99.5%) and 50 ml of glycerol, chemically pure, are added and mixed well. Filtration is unnecessary. This solution keeps indefinitely in a closed container at room temperature. The smear examined with either method should be examined under
oil-immersion lens. The tubercle bacilli appear as dark-red dots in a blue or
green background. Concentration Method Mix equal volumes of sputum and sodium hypochlosite 5.25%. Centrifuge the mixture at high speed for 10 minutes. Pour off the supernatant and drain the tube for 2 minutes. Transfer the sediment to the slide, fix and stain the smear with AFB stains. 2. Gram's staining 3. Capsule staining (i) Smith's method (ii) Hiss' method The organisms frequently
encountered are mycobacterium tuberculosis, staphylococci, streptococci,
Diplococcus pneumonie, Mebsiella pneumoniae Haernephillus influenzae,
Haemophillus pertussis, and neisseria. LIVER FUNCTION TESTS Indications Shortcomings (ii) Some tests may be positive in extra hepa tic lesions. Classification
I. Tests based on bile
pigment metabolism: Bilirubin may be present in conjugated or unconjugated form. The two types
of bilirubin can be distinguished by van den Bergh's test. Ehrlich's
diazoreagent is added to serum of the patient. Red colour indicates
directpositive test (conjugated). If this red colour deepens on addition of
alcohol, the test is biphasic (mixed). If the colour appears only on addition
of alcohol the test is indirect positive (unconjugated). 2. Bile pigment and salt in urine: 3. Estimation of urobilinogen in urine: Normal
0.5 - 3.0 mg/day II. Test based on
excretory functions of liver: Bromsulphthalein
retention test:
III. Test based on detoxication: Benzoic acid conjugation
test. IV. Tests based on metabolism: 1. Carbohydrate
metabolism: 2. Protein metabolism: (i) Estimation of
total proteins: (a) Cephalin cholesterolflocculation test. The result is expressed as: Normal : 0, + Positive : ++, +++, ++++ (b) Thymol turbidity test
(c) Zinc sulphate
turbidity test: Caution. These tests may also be positive in other conditions with hyperglobulinaemia, e.g., kalaazar, malaria, multiple myelosis, sarcoidosis and collagen diseases. (iii) Estimation of serum prothrombin level. A low serum prothrombin level, not improving after administration of vitamin K, shows liver damage. 3. Serum Cholesterol
150 - 250 mg/100 ml. Raised in obstructive
jaundice (exclude V. Tests based on enzyme synthesis: 1. Serum alkaline phosphatase: Produced by liver
osteoblasts. (i) Obstructive jaundice. (ii) Space occupying lesions of the liver. Lowered in Severe liver damage. 2. Serum glutamic oxaloacetic transaminase (SGOT) Normal 5-40 units. Raised in The level is raised in proportion to the extent of damage. However, myocardial damage should be .excluded. 3. Serum glutamic pyruvic transaminase (SGPT). Normal 120-500 units Importance of Enzyme
Tests: VI. Test based on hormonal regulation: Urine Ketosteroid
Estimation: VII. Test based on a absorption and storage of iron. Estimation of Serum Iron: Normal 80-140 mg.
per 100 ml. Selection of Tests Jaundice: Serum bilirubin estimation with van den Bergh reaction Serum alkaline phosphatase Sero-flocculation test (iv) Serum cholesterol (v) Urinary and faecal urobifinogen (vi) Bile salts and pigment in urine. Hepatitis (a) Pre-icteric: (b) Icteric: (i) Bile pigment in
urine (i) Bile pigment and
urobilinogen in Liver Cirrhosis., (i) Seroflocculation
Neoplasms and space occupying lesions: - Serum enzymes. RENAL FUNCTION TESTS
Diurnal Variations The patient should not take water after 6 PM. Urine is collected between 10 PM and 6 AM and specific gravity measured. In normal persons, the specific gravity is 1023 or above. In kidney diseases, specific gravity is lowered and the amount of urine passed during night may approximate to that during the day. Other conditions to be differentiated are: (i) Diabetes insipidus
Water Clearance Test First, take a sample of urine emptying the bladder completely. After one hour ask the patient to take one pint of water. Collect the urine hourly for 3 hours. Measure the amount and specific gravity of every sample. In normal persons, there is quick diuresis; within 4 hours, most of the water passes out. Damaged kidneys cannot remove the extra load of water. Urea Concentration Test The patient is not given water for 10 hours. Then he is given 15 G of urea dissolved in 150 ml. of water and flavoured with suitable agent. Urea is estimated in the urine every hour for 3 hours. In normal persons at least one sample should contain minimum 2.5 G of urea per 100 ml. PSP Test The advantage is that inefficiency of single kidney can be tested. The substance is harmless, non-irritant, excreted freely by the kidneys, and easily detected in urine. 300 ml. water is given and bladder emptied. One mi. of dye solution containing 6 mg. of PSP is injected intramuscularly. Urine is collected in a test tube containing some alkali. If two separate catheters are used, the function of individual kidneys can be tested. Appearance of dye in the urine manifests by red colour. In normal persons, the dye appears within 10 minutes; 40-60 per cent of the dye is excreted in first hour, and 20-25 per cent in second hour. Total excretion of less than 50 per cent indicates renal damage. Congo Red Test In normal persons, only 40 per cent of the dye disappears from the blood in an hour. In renal amyloidosis, the dye disappears very quickly. Urea Clearance Test Urine is collected and measured for a period of 2 hours, with or without loading the urine. Sample of blood is taken at the mid-point of collection period. Amount of urine passed per minute is calculated. Urea clearance is calculated as follows:.
UxV
U x V Where Cm. or Cs
is the urea clearance, U the amount of urea in the urine, V the volumeof
urine passed per minute, and B the blood urea. If the volume per minute is
more than 2 ml. maximum urea clearance (Cm) is calculated the normal value
being 65.85. If the volume per minute is less than 2 ml., standard urea
clearance (Cs) is calculated; the normal value being 44.64.
Creatinine Clearance Test The excretion of urea is the resultant of glomerular filtration and tubular reabsorption. Creatinine, however, is not reabsorbed by tubules and thus has an advantage in the clearance studies. Normal value is 90-100 per cent. Inulin Clearance Test Inulin is completely filtered off and completely unchanged by the tubules. Normal value is 100 per cent. Blood Urea Estimation Normal blood urea level is 20-40 mg per 100 ml. It is unaltered in the early stages of chronic nephritis but later, there is a marked rise. In terminal stages, it frequently exceeds 500 mg. per 100 ml. The extrarenal conditions to be differentiated are:
Blood Creatine Estimation Normal 0.8-1.0 mg per ml. Not affected by protein intake. Blood Uric Acid Estimation Normal – Female : 2.4-6.0 mg/dl Male : 3.4-7.0 mg/dl Raised in (iii) Gout. Plasma Proteins Normal serum protein 6-7.5 G/100 ml. (Albumin 3.3-5.5 G; globulin 2.3-3.0 G). Serum albumin below 2.5 G1/100 ml. leads to oedema; Albumin: globulin ratio is reversed. Serum Cholesterol Normal - 150-250 mg/100
ml. CSF EXAMINATION Components of CSF examination
Physical examination 1. Pressure:
2. Appearance: Turbid in pyogenic meningitis Cob-web coagulum in tuberculous meningitis. Blood: (a) Trauma of needle (b) Intracranial haemorrhage (c) Subarchnoid haemorrhage. Xanthochromia: (a) Spinal block (b) Auditory nerve tumour (c) Chronic jaundice (d) Polyneuritis. Chemical Examination 1. Proteins
5.
Chlorides: Raised in: Uraemia. Lowered in: (a) Purulent meningitis (b) Tuberculous meningitis. 3. Sugar: Normal 50-80 mg/100 ml Absent in: Pyogenic meningitis Reduced in: Tuberculous meningitis Normal in: Viral infections. Cell-Count Normal 0.5 cells/cu. mm. (usually lymphocytes). 5-100 cells/cu. mm. in: (a) Neurosyphilis (b) Encephalitis (c) Poliomyelitis. 100-500 cells/cu. mm. in: (a) Tuberculous meningitis (b) Syphilitic meningitis (c) Aseptic meningitis. Beyond 500 cells/cu mm. in: - Purulent meningitis. Causes of lymphocytosis in CSF: (a) Neurosyphilis (d) Tuberculous meningitis (e) Cerebral tumour (f) Lymphatic leukaemia (g) Chloroma. Causes of Polymorphonuclear leukocytosis in CSF: (a) Pyomeningitis (b) Poliomyelitis (early stages). Bacteriology Gram positive cocci
: Pyogenic meningitis Special Investigations (i) Colloidol gold test: Depends upon proportion of α-globulin and other proteins. α-globulin precipitates colloidal gold whereas albumin and β-globulin inhibit it. Serial dilutions of CSF are prepared with a solution of colloidal gold and allowed to stand overnight. Normal CSF does not show precipitation. Precipitation indicates three types of patterns :- (a) Paretic pattern.
Maximum precipitation in the tubes containing high concentration of CSF
(b) Leutic
pattern. Precipitation in the tubes with relatively less concentration of CSF (c) Meningitic
pattern. Precipitation in tubes with least concentration of CSF (ii) Pandy's test. Depends upon the precipitation of globulin by aqueous phenol. Positive in meningitis Slightly positive in neurosyphilis. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||














|
Chapter 2 : Haematology BLOOD FORMATION (HAEMOPOIESIS) Blood formation takes place from primitive tissue or mesenchyme. From the early foetal life till late adult stage the location of blood forming mesenchyme, changes with regular transition. 1. The earliest site of blood formation is area vasculosa which comprises islands within the mesenchyme of yolk sac. The intravascular primitive cells are termed haemocytoblasts or haemohistioblasts. This phase continues to 9th week of intrauterine life. 2. In the second month of intrauterine life blood is formed predominantly in the liver. During 5th month, blood formation begins also in spleen and thymus. The splenic activity subsides shortly and during the last three months of foetal fife only hepatic activity continues slowly giving way to bone marrow as blood forming organ. 3. During the last trimester of intrauterine life, blood formation starts in the bone marrow; by the time of birth, bone marrow takes up this function completely. 4. During adult life haernopoiesis gets gradually restricted to red bone marrow in vertebrae, ribs, sternum, skull, pelvis and proximal epiphyseal regions of the humerus and femur. Till puberty all the marrow in all the bones is red and blood forming; later it becomes yellow, fatty and inactive blood forming sites. Under conditions of stress as in haemolytic anaemias when excessive blood formation is imperative, the fat in the yellow bone marrow disappears rendering it red and active again; haemopoietic activity of liver and spleen also revives but not of thymus. Development of Red Blood Cells The common precursor of red blood cells,'polymorphs, eosinophils, monocytes and platelets is stem cell. Whether stem cell is also the precursor of lymphocytes is disputed. Under the influence of enzymes erythropoietin, granulopoetin and thrombopoietin, the stem cells get differentiated into erythroblast (normoblast), granulocytoblast and thrombocytoblast. There are four stages in the development of red blood cell: 1. Pronormoblast
2. Basophilic normoblast
(Early normoblast) Polychromatic normoblast (Intermediate normoblast) (i) Irregular outline.
4. Orthochromatic normoblast (Late normoblast) (i) Spherical in
shape. Orthochromatic normoblast, after complete disappearance of nucleus is termed reticulocyte or juvenile red blood cell. It still has the remnants of basophilic RNA. The stages of erythropoiesis described above appear in the bone-marrow and it is the mature red blood cells which appear in the peripheral blood. However, normoblasts can be observed in peripheral blood smears in cases of severe anaemias and leukaemias. Reticulocytosis The normal reticulocyte count is 0.5-2.0% of the red blood cell count. High reticulocyte count (reticulocytosis) indicates excessive generation of red blood cells as seen in: 1. Physiological (i) Foetal life (iii) Spring season (iv) Pregnancy. Pathological CLASSIFICATION OF ANAEMIAS I. On the basis of size of
red blood cells: Il. On the basis of
mean corpuscular haemo 1. Hypochromic III. On the basis of etiology: A. Excessive loss or
destruction 2. Intravascular (Haemolytic) (i) Congenital (ii) Acquired. B. Failure of output
2. Hypoplastic or aplastic (i) Primary (ii) Secondary. MEGALOBLASTIC ANAEMIA Maturation of red blood cells depends upon extrinsic factors viz. vitamin B,,, folic acid and an intrinsic factor in the gastric juice, believed to be an enzyme, haemopoietin. The intrinsic factor helps in absorption of the extrinsic factor. The deficiency of intrinsic factor is often hereditory the condition being known as pernicious anaemia. Causes of Megaloblastic Anaemia Inadequate intake of vitamin B12 and folic acid. Defective absorption:
3. Excessive demand
The Megaloblasts
Chart : Erythropoiesis
In the deficiency of
vitamin B12 and folic acid the blast stages of red blood cells are
abnormally larger and are termed megaloblasts (cf, normoblasts). Just as
normoblast, megaloblast also develops in four stages viz. 2. Basophilic megaloblast (i) 13-22µ in diameter (ii) Chromatin reticular without nucleoli (iii) Cytoplasm intensely basophilic. 3. Polychromatic megaloblast (i) 12-20µ in diameter (ii) Chromatin reticular (iii) Cytoplasm polychromatic or eosinophilic. 4. Orthochromatic megaloblast (i) 10-17 µ in diameter with distorted shape (ii) Nucleus small and eccentric (iii) Nucleus shows clumping (iv) Cytoplasm abundant and eosinophilic. The orthochromatic orlate megaloblasts appear in peripheral blood smears in pernicious (and other megaloblastic) anaemia. Pernicious Anaemia Pernicious anaemia is a
type of megaloblastic anaemia in which absorption of vitamin B12 is
hampered due to chronic atrophic gastritis and the resultant failure of
release of intrinsic factor.
Blood Picture Bone Marrow Changes 1. Very marked
erythroblastic reaction Other Diagnostic Aids 1. Serum bilirubin
raised with an indirect van den Bergh's reaction. IRON DEFICIENCY ANAEMIA Etiology
Blood Picture
1. Mean corpuscular
volume 50-70 cuµ (microcytic). Bone Marrow 1. Normoblastic
hyperplasia Other Changes 1. Serum bilirubin
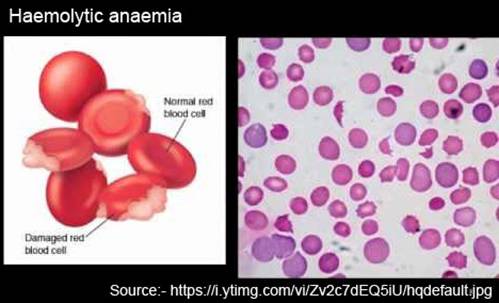
low with no evidence of increased haernolysis. HAEMOLYTIC ANAEMIA Classification (Depending upon the causes)
Blood Picture
1. Erythrocytes
normocytic or microcytic in chronic cases, macrocytic Blood Marrow
Other Changes 1. Serum folic acid low.
ABNORMAL HAEMOGLOBINS The normal form of haemoglobin in the adult has beeii designated as 'A' and that in the foetus as 'F' Genetically distinct abnormal forms of haemoglobin occur as a result of small molecular abnormalities. The most striking example is haemoglobin-S. In the homozygous forms (with abnormality in both chromosomes of a pair), fatal forms of haemolytic anaemia appear such as sickle cell anaemia and thalassaemia. Detection The following tests, the first two of which are briefly described here, are usually employed. 1. May-Grunwald's stain. This method is employed in detection of foetal cells which appear as pink staining refractile cells. 2. Alkali denaturation. When oxyhaemoglobin is treated with alkali, a brownish material (alkaline globin haematin) is formed. The reaction involves oxidation of haem iron to the ferric state, as well as denaturation of globin. The proportion of haemoglobin which does not undergo denaturation is termed as alkali resistant. If time is prolonged the whole haemoglobin undergoes denaturation. Denaturation of normal adult haemoglobin takes place within one minute. A one-minute denaturation value represents the percentage of alkaliresistant haemoglobin. A value of 03-1.7 per cent is normal. Values above 2 per cent are taken as abnormal. 3. Paper electrophoresis.
Common
Haemoglobinopathies Sickle-cell Anaemia In the heterozygous state (only one chromosome involved out of a pair), the condition is termed sickle cell trait.
In sickle cell anaemia, there is marked anaemia and leucocytosis. The total erythrocyte count averages 2 million/cu. mm. and total leucocyte count 20,000/cu. mm. The film shows an extraordinary change in the shape of red cells; large number of these are of crescentic, sickle or stellate form. Many of the abnormal cells are being phagocytosed by macrophages. Reticulocytes are increased. The serum is deep yellow due to great increase of bilirubin. In sickle cell trait blood appears to be resistant to falciparum malaria. Thalassaemia It is a haemolytic anaemia due to an inherited abnormality of haemoglobin. Foetal haemoglobin continues to be produced after birth. The homozygous condition is almost always fatal in early life. The disease occurs in two forms viz. Thalassaema major (homozygous) and thalassaemia minor (heterozygous). Thalassaemia major (or Cooley's anaemia) is fatal in infancy and childhood. The blood may contain 40-100 per cent of foetal haemoglobin. There is a severe microcytic, hypochromic anaemia with much anisocytosis, poikiolocytosis, elongated and oval cells, and large number of characteristic target cells and leptocytes. Reticulocytes may be upto 30%; stippling, Howell-Jolly bodies and cabot rings are commonly found. Total leucocyte count is raised (13,000-50,000/cu. mm), with a few myeloid cells in more severe cases. The van den Berg reaction is indirect positive and the icteric index is raised. Blood platelets are usually normal.
Thalassaemia minor (Retti-Greppi-Micheli syndrome) and even minor grades known as thalassaemia minima, which arise from heterozygous inheritance, are mainly symptomless. A chance examination reveals mild anaemia with typical haematological features. APLASTIC ANAEMIA Aplastic anaemia is a type of pancytopenia (reduction in all types of blood cells) characterised by a normocytic, normochronic anaemia, neutropenia and thrombocytopenia. Rarely there may be only an erythroid aplasia, the condition being known as pure red cell aplasia. Causes
Blood Picture
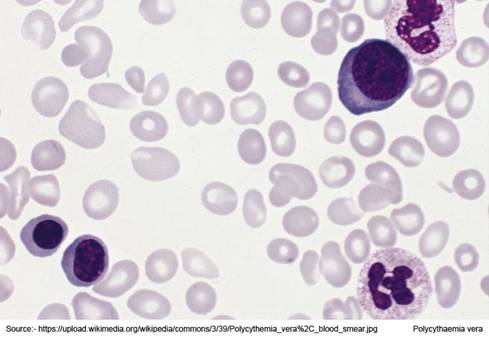
1. Normocytic normochromic anaemia 2. No evidence of erythropoiesis such as polychromatophilia, and reticulocytosis 3. Leucocyte count low, may drop below 1,000/cu. mm., mainly lymphocytes present 4. Platelet count low 5. Serum iron elevated to the saturation of total iron-binding capacity. Bone Marrow Aplastic or hypocellular bone marrow; in the initial stages it may occasionally be hypercellular. POLYCYTHAEMIA An increase in the number of circulating red blood cells, is termed polycythaemia. Causes
Polycythaemia Vera Blood Picture
1. Total erythrocyte count
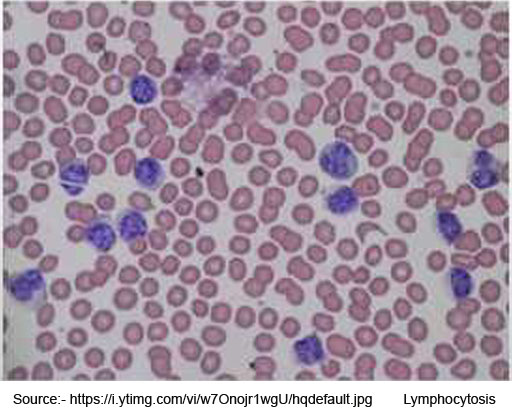
7-12 million/cu mm Bone Marrow LEUCOCYTOSIS The normal total leucocyte count is 5000-8000/cu. mm.
Counts below normal are termed leucopenia whereas the counts above normal are
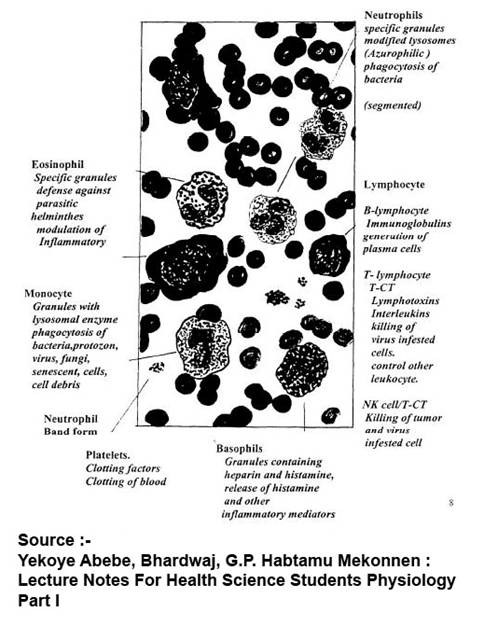
termed leucocytosis Blood Cells
Granulocytes Physiological leucocytosis 1. Pregnancy 2. After meals 3. After exercise. Types and Causes A. Neutrophilic leucocytosis (mainly in acute infections):
B. Lymphocytosis
C. Eosinophilia
D. Monocytosis
E. Basophilia
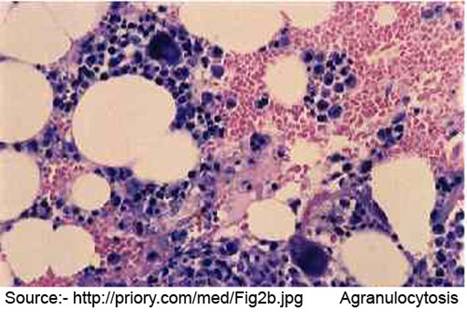
NEUTROPENIA (AGRANULOCYTOSIS) An abnormally low white cell count is termed leucopenia. Any type of white cells may be reduced. An uncommon variety in which lymphocytes are reduced is termed lymphopenia, generally associated with Hodgkin's disease, non-lymphocytic leukaemias, corticosteroid therapy, and occasionally with chronic diseases. The commonest variety of leukopenia is neutropenia in which neutrophils (polymorphs) are reduced in the circulating blood. Neutropenia of higher grades which has serious consequences by predisposing to infections is termed agranulocytosis. Causes
Pathology 1. Bone marrow initially hyperplastic but in 2-3 days becomes progressively hypocellular, may be completely devoid of myeloid elements although erythroblasts and megakaryocytes are almost normal. 2. Ulcerating necrotizing
lesions of the gingiva, floor of the mouth, buccal mucosa, pharynx or anywhere
in the oral cavity (agranulocytic angina); the ulcers are typically deep,
undermined and covered by gray to green black necrotic membranes from which
number of bacteria or fungi can be isolated. Severe necrotizing infection may
also be present in the lungs, urinary tract, and kidneys. Blood Picture
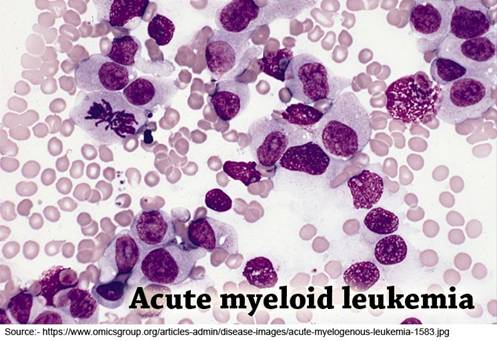
3. Leucocyte count low; polymorphs may be entirely absent; total count generally less than 1,000/cu mm., absolute lymphocyte count and absolute monocyte counts also reduced though percentage may be high. An increased absolute monocyte, count indicates favourable prognosis. LEUKAEMIA Leukaemias are a group of myeloproliferative diseases characterized by a remarkable increase in the blood leucocyte count which does not correspond with that of a reactive leucocytosis. Classification
Chronic Myeloid Leukaemia Blood Picture
3. Platelets. Unchanged
initially; increased later Bone Marrow
Chronic Lymphoid Leukaemia Blood Picture
Bone Marrow Acute Myeloblastic Leukaemia Blood Picture
Bone Marrow Acute Lymphoblastic Leukaemia Blood Picture
1. TLC.
10,000-500,000/cu. mm. (average 70,000/cu. mm) Acute Monocytic Leukaemia Blood Picture
LEUKAEMOID REACTIONS Leukaemoid blood reactions are the nonleukaemic conditions with peripheral blood picture resembling that of leukaemia. There may be marked elevation of total leucocyte count or the presence of immature leucocytes, or both. The leukaemoid reactions may be either myeloid or lymphatic. Generally only one type of reaction is caused by a particular disorder but some disorders such as tuberculosis, carcinoma may cause either of the two types. Causes
Leukaemoid Reaction v/s
Leukaemia
HAEMORRHAGIC DISORDERS Classification
IDIOPATHIC THROMBOCYTOPENIC PURPURA Etiology. Cause not exactly known; generally believed to be immunologic. Most patients have autoantibodies against platelets and causing platelet destruction as evidenced by the following facts: 1. Infants born to
affected mothers are often thrombocytopenic. Pathology 1. Spleen Microscopic 2. Blood picture
HAEMOPHILIA Haemophilia is a hereditary disease affecting males but transmitted by females and characterised by prolonged coagulation time and a lifelong tendency to excessive haemorrhage due to a quantitative deficiency of andhaemophilic globulin. True haemophilia may occur occasionally in a child with no previous family history because of mutation. The disease has also been recorded in one of a pair of identical twins. Thus it is evident that by union of a carrier female and a normal male, the progency will include a normal male, a carrier female, and a haemophilic male. Similarly a carrier female
may be produced by normal mother and a haernophilic father, the transmission
being represented in the following chart: The few recorded cases of haemophilic females are the result of union of a haemophilic male and a carrier female, the chances of which are virtually nil. In haemophilia, there is
no significant change in the corpuscular elements of the blood the number of
polymorphonuclears is some what diminished. The platelets in shed haemophilic blood are much more slow to undergo vicious metamorphosis than those of normal blood. This is due to the absence of the specific antihaemophilic globulin (AHG) known as factor Vill. This antihaemophilic globulin normally promotes the disruption of platelets which come in contact with an abnormal surface and thus initiates the process of clotting by the formation of blood thromboplastin. Accordingly failure of coagulation in haemophilia depends on lack of formation of the thromboplastin. The tendency to occurrence of serious effusion and haemorrhages into the joint in haemophilia points to the co-existence of some vascular abnormality. Christmas disease (Haemophilia B) is due to deficiency of factor IX, plasma thromboplastin component (PTC) in the absence of which thromboplastin formation fails and a haemorrhagic disorder clinically identical with haemophilia results. It shows a similar sex linked inheritance. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||















|
Chapter 3 : Inflammation & repair INFLAMMATION
Causes of Inflammation
Acute
Inflammation
Causative Irritants
.
The foreign body giant cell is larger than an
ordinary cell and may be of enormous size. It contains numerous nuclei,
sometimes as many as 50-100. The nuclei, are regular in size, seldom large
and are scattered through the cytoplasm. However, in certain conditions e.g.
tuberculosis the nuclei may be arranged around the periphery (Langerhan's
giant cells). Foreign body giant cells are seen in; The third group 'miscellaneous'
include the giant cells of mesodermal origin e.g. Aschoff cells of rheumatic
nodule. Another member is the Reed-Strenberg cell of Hodgkin's disease.
Chemical mediators of acute inflammation
The above mediators subclassified on next screens
RESOLUTION Resolution is the process of retrogression of the various phenomena occurring in inflammation. There is a tendency to restoration of normal blood flow and absorption of exudate. As the irritant is removed from the tissue or otherÂwise its effect
countered, the stagnation passes off and the blood flow is restored though a
certain amount of vascular dilatation often persists for some time. The
exudate if fluid, is absorbed chiefly by lymphatics and fibrin is digested by
leucocytes and thereafter absorbed. If however, the fibrin is abundant or
dense, its absorption is effected only after the ingrowth of fibroblasts and
capillaries, i.e., by a process of organization. This is the common result in
the case of a fibrinous exudate on a serous membrane. Connective tissue cells
which have become swollen and separated in an inflamÂmed part diminish in
size and become attached again to fibres or form new fibres. The defects in
endothelial lining may be completely restored by surviving cells. Healthy
leucocytes may pass back through the endothelium of the vemiles to the blood
stream; but those that are damaged and also the extravasated red cells are
either taken up by phagocytes or are carried by the lymph to the lymph nodes,
where they are similarly dealt with. The phagocytes are macrophages
developing from both the monocytes and cells of local origin (histoÂcytes).
Within a macrophage, sometimes several polymorphonuclear leucocytes are seen.
The phagocytosed leucocytes are gradually digested and disappear. Damaged red
corpuscles are also taken up by these phagocytes and destroyed.
. Cell Cycle
Phases
CHRONIC INFLAMMATION Chronic inflammation is the response of body tissues to the persistent traumatic stimuli.
Causes
Infective organisms (i) Mycobacterium tuberculosis (ii) Treponema pallidum. Mild poisons in solution - Lead. Particulate irritants (i) Silica dust (ii) Vegetable cells (iii) Lime salts (iv) Pigments.
Pathogenesis
Chronic inflammation in various organs may occur in three ways: 1. It may follow an episode of acute inflammation where the inciting stimulus persists in the body. 2. There may be repeated attacks of acute inflaÂmmation with healing phase in between as in cholecystitis and pyelonephritis. 3. Chronic inflammation may develop as a priÂmary entity without a preceding attack of acute inflammation, as in rheumatoid arthritis tuberculosis, chronic bronchitis. Pathology The characteristic features of chronic inflammation are: Emigration of mononuclear cells is an important component of chronic
inflammation. The monocyte, on reaching the extracellular tissue, gets
changed into a much larger cell, the macrophage. Macrophages accumulate in
large numbers in three ways. The various types of chronic inflammatory lesions have some relatively distinguishing features in the structure, however, they are not always specific. The tubercle follicle is characteristic of lesions due to Mycobacterium tuberculosis, but this organism may at times produce a quite different and much more acute exudative lesions in the meninges or pleura. Also the Treponema pallidum commonly induces a diffuse chronic inflammatory response, but at times in older lesions, a markedly folficular character may be seen and an erroneous diagnosis of tuberculosis may then be made. Tubercle folliÂcles are also very characteristic of sarcoidosis and are frequently induced in the tissues by foreign bodies. Effects of Chronic Inflammation 1. Contraction of newly formed tissue leads to narrowing of orifices
and tubes, e.g. 2. Uneven affection of interstitial tissue results in coarse granularity of the surface, e.g., in chronic pyelonephritis. 3. Loss of parenchymal cells of the organ. 4. Replacement of specialised connective tissue by more resistant connective tissue cells, e.g., in liver cirrhosis. ABSCESS An abscess is a localised collection of pus caused by suppuration burried in a tissue, organ, or confined space. Formation of Abscess Abscesses are usually produced by the deep seedÂing of pyogenic bacteria
into a tissue. Two chief changes occur inside the tissues viz. 2. Gradual destruction and disappearance of the tissue
elements. The progressive emigration of leucocytes is due to a continued supply of
chemotactic substances from the bacteria. Although the pyococci are most freÂquently
concerned, suppuration may be produced by a great variety of organisms, the
essential point being that they should be able to persist in the tissues and
produce their effects. Digestion and liquefaction of the tissue is chiefly
due to proteoÂlytic enzymes produce by leucocytes. Certain pyoÂgenic
organisms have a digestive action of proteins but others e.g. steptococci and
pneumococci have no such property. Digestive softening of the tissue by
leucocytes follows damage or actual necrosis due to bacterial toxin, as there
is no evidence that leucocytes, however numerous, will attack normal tissues.
Digestivc action by the leucocytes is seen also when suppuration is preceded
by much exuÂdation of fibrin, e.g., in pleurisy. The fibrin is to a large
extent digested and disappears and this is closely analogous to the action of
leucocytes in removing fibrin in the process of resolution of inflammation as
seen in pneumonia. In dense tissues, complete suppurative softening may fail
owing to the density of the tissue. A portion of dead tissue or slough then
forms and may persist for considerable time.
Subsequent Fate When suppuration ceases to spread, at the periÂphery of an abscess, a reactive proliferation of the connective tissue cells with new formation of blood vessels forms a zone of granulation tissue around it. The outer part of it becomes denser and a definite wall to the abscess is formed (pyogenic membÂrane). If the abscess is of small size, the pus may be absorbed and a smaller scar results. The pus may, however, be too abundant for this to occur. Then it becomes thickened and changed into granular debris. In this debris lime salts may be deposited. When an abscess forms near a free surface as in subcutaneous tissue, the tension of the contents causes the suppuration to extend in the direction of surface so that the overlying skin is involved. The abscess is then said to "point". It may ultimately discharge its contents spontaneously. HEALING AND REPAIR Healing Factors Affecting Wound Healing A. General factors 1. Age. Healing is quickest in children. As the age advances, the process is impaired due to comparatively less blood supply. 2. Nutrition. The nutritional state of the patient, particularly the protein intake is of utmost importance. Serious protein deficiency with hypoproteinaemia and oedema predisposes to prolonged and complicated wound healing. 3. Vitaniin C. It is necessary for the formation of intercellular substance and maturation of collagen of connective tissue. 4. Vitainin K Vitamin K deficiency with hypoÂprothrombinaemia and a bleeding tendency may interfere with normal wound healing by the formation of haematomas and scrum collection. These in turn predispose to wound separation and wound infections. 5. Vitainins A, D, and B-complex. Their deficiency lowers the rate of
phagocytosis and bacterial digestion, thus predisposing to local wound
infection. 3. Haematomas and serum collections. 4. Ischaemia. 5. Foreign bodies. 6. Desiccation of the tissues. 7. Improper approximation. Healing in a Clean Incised Wound In a simple incised wound such as is made in asepÂtic surgery, the process of healing is simple and rapid. Such a wound is said to heal by primary union. When bleeding has been arrested and the margins have been fixed in apposition, the adjacent surfaces are glued together with a thin layer of coagulum. There is a slight degree of congestion of the superficial vessels with some liberation of plasÂma which coagulates, but ordinarily this is scanty and only a few leucocytes emigrate from the vessels into the clot. Within a short time the connective tissue cells become swollen and divide by mit ' osis. This cells in the form of fibroblasts, migrate into the thin layer of coagulum, which undergoes absorption by the action of these cells and of leucocytes. Capillary bands accompany the fibroblasts, but often little vascularisation is necessary. The fibroÂblasts from adjacent sides become intermingled; they arrange themselves At right angles to the line of wound and produce the collagen fibrils which bring about the permanent union. At the same time the epithelial cells grow over the line of incision from the two sides and restore the continuity of epithelial covering. At the end of 5-6 days the proÂcess is practically completed and. only a narrow band of young connective tissue remains to mark the line of incision. If the wound surface has been irritated or if the wound has been a large one, serous discharge from the vessels may be considerable. In such a case the emigration of leucocytes continues for a longer time and formation of fibroblasts and new capilÂlaries is likewise of longer duration and more abundant resulting in a more distinct line of fibrous tissue than in the case of simple aseptic healing. Healing in an Infected Wound Healing process in an infected wound is by granulation tissue and is
termed secondary union. It consists of two parts: 2. Replacement or reconstruction of the original tissue, as far as possible. It involves the invasion and replacement of dying and dead tissue by
immature mesenchyme called granulation tissue. The process commences at the
base and works to the surface, so that the youngest tissue is always at the
surface. Such a surface is highly vascular and bleeds very readily. On account of its cellularity a granulating surface has a remarkable power
of resisting bacterial infection. It presents so powerful a barrier that
septicaemia cannot occur once an intact wall of granulation tissue has been '
formed. The granulation tissue grows in duly from below upwards. In the
superficial layers the fibroblasts run at right angle to the surface and
therefore parallel to the When the surface is covered by epithelium the proÂcesses of devascularisation begins. The new vessels gradually disappear and the scar which is first red becomes white and bloodless. Repair Repair of Fracture When a bone undergoes a simple fracture, there is necessarily tearing of blood vessels and of soft tissues and a varying amount of haemorrhage occurs between the broken ends. The periosteum is usually torn through and separated from the bone to a varying extent in the neighbourhood of the breach. Bleeding soon ceases and coagulation of the effused blood occurs. Soon there follows reaction on the part of the vessels. There is exuÂdation from them which leads to a swelling ofthe tissues at the site. The process of repair begins by proliferation of cells and formation of new blood vesseles. The proliÂferation takes place in cells of the endosteum and of the deep or cambium layers of the periosteum as well as in cells derived from the bone especially from the Haversion canals. All these cells posses osteogenic function, i.e., are osteoblasts. The new blood vessels accompanied by the cells grow out from the pre-eidsting blood vessels and make their way into the clot which gradually becomes replaced by a cellular and vascular tissue. In this newly formed tissue the young bone cells, the steoblasts have branching processes from which delicate fibrils pass in all directions. In the process of bone formation, the young bone cells and the fibrils are seen to become enclosed in a somewhat homogeneous matrix forming trabeculae of osteoid tissue which become osseous (bony) tissue by deposit of lime salts. The newly formed bone has a somewhat spongy character, and it comes to enclose and unites the ends of the fractured bone. It is then known as provisional callus. The callus is sometimes artificially divided into an internal callus in the medullary cavity, an interÂmediate callus between the ends of the bone, and an external callus outside. The amount of callus varies very much in different cases and is least abundant in case of simple fractures. While the newly formed tissue is mainly a vascular osteoid and osseous tissue, islets of young cartilage may also develop especially when there has been much movement. Provisional callus is formed rapidly and serves to bring about early union. The next stage is one of strengthening the union and adapting the configuration of the bone to the functional requirements. Parts of the callus are penetrated and resorbed by the new blood vessels surrounded by osteoblasts and these cells then lay down bone by lamellar apposition in the form of Haversian systems. This process goes on till a more compact type of bone is produced, which forms the permanent union; this is known as the definitive callus. The external callus is to a great extent absorbed so that if there has been a proper apposition, the configuration of the bone is largely restored. When a bone has been united in a wrong position, the newly formed bone is not only more abundant but is arranged and moulded in a striking way, according to the muscular requirements. The repair of the compound fracture proceeds in a similar way but entry of organisms may cause suppuration and may interfere with formation of callus sometimes leading to resorption of callus already formed. When there is exit for pus the healing takes place very much as in a granulating fracture would. There is an advancing line of ordinary granulation tissue behind which granuÂlation goes on and ultimately and space occupied by pus maybe obliterated and the process of bone formation may be completed. Just as in soft tissues, where long continued, suppuÂration produces much overgrowth of fibrous tissue, so in the case of compound fracture there may be considerable and irregular formation of new bone. When a sequestrum is present, it becomes a nidus for organismal growth, pus forms around it; suppuration may in this way, be kept up for an indefinite period of time, the pus being discharged from the sinus which leads down to the dead bone. Causes of Delayed Union
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||




|
Chapter 4 : Circulatory Disturbances THROMBOSIS
Clotting of the blood inside a vessel during life is termed thrombosis. Thrombosis is essentially a platelet deposition. Types of Thrombosis Thrombosis is classified according to its site: Common site is the deep veins of calf muscles. 2. Arteries. Common in the (i) Coronary artery (ii) Cerebral artery (iii). Aorta (iv) Femoral arteries. 3. Heart. Found in (ii) Left ventricle (iii) Left auricle. 4. Capillaries. Occurs in (i) Sickle cell anaemia (ii) Malaria. Causes of Thrombosis There are three factors described as Virchow's triad. 1. Slowing of blood stream. More common in veins due to slow blood flow, commonly seen as postoperative complication in patients with an ageing heart muscle. Common in congestive heart failure especially when combined with confinement to bed. Normally platelets flow in central portion of the stream. As the stream becomes slow they flow in the peripheral portion. 2. Changes in the vessel wall. Injury to the intima may occur in the arteries, the veins or the heart. In the arteries, the smooth intima may be roughened by atheroma which also narrows the lumen and retards the stream. It may become necrotic as a result of malignant hypertension, periarteritis nodosa and disseminated Jupus erythematosus. The veins are liable to injury by trauma, by pressure and by injection. In the heart, valves are injured by inflammation so that thrombi are deposited on the surface. 3. Changes in the blood (iii) Increased viscosity of blood in polycythaemia. Mechanism of Thrombosis
. If a vessel wall is merely damaged, thrombosis may not occur, but if at the same time damaged part is projected inwards, the platelets are brought into contact with its surface to which they adhere, heaping themselves up and in this way starting a thrombus. Complications of Thrombosis When a pure thrombosis is completely successful in its function, it is clinically silent. When complicated by clotting it may or may not become clinically manifest. The following effects may be produced depending upon the site of thrombus, the type of vessel involved and the degree of occulsion: 1. Oedema of a limb. Occurs when venous thrombosis is complicated by
perivenous lymphangitis. 5. Infarction of the myocardium, retina, etc. due to arterial
thrombosis. Ultimate Fate (Sequelae) of Thrombosis 1. Fiblinolysis. Restoration of the vascular channel after
thrombotic occlusion may occur by a combination of fibrinolysis and shrinkage
of the thrombus. The fibrinolytic mechanism depends Types of Emboli upon the
activation of pIasminogen in the plasma A. Depending upon physical state, the
emboli may and this may become very active when there has 2. Organisation. The thrombus becomes permeated by young connective tissue cells and capillaries, the later growing in form the vasa vasorum and from the intimal endothelium. Its substance becomes gradually absorbed and 2. ultimately replaced by connective tissue. In some instances, the young vessels that grow in from the vascular endothelium covering the thrombus anastomose and then enlarge to form new channels by 3. which the thrombus is said to be canalised. 3. Infection. Venous thrombi may become infected with pyogenic organisms and may then undergo suppurative softening so that portions are carried away by blood stream and give rise to abscesses in other parts of the body producing pyaemia. Thrombosis v/s Coagulation
EMBOLISM Partial or complete obstruction of some part of cardio-vascular system by a foreign body transported by the blood stream is termed embolism. Types of emboli Depending upon physical state, the emboli may be: (ii) A mass of tumour cells (iii) Parasites. 2. Liquid: (i) Fat globules (ii) Amniotic fluid. 3. Gas - Air. B. Depending upon the site, the emboli may be: Mode of Formation B. Liquid emboli 2. Amniotic fluid embolism may occur during or immediately after labour. Fluid may enter through tears or during rupture of membranes through venous sinuses of the uterus. C. Air emboli Occur in: 1. Operations on neck ISCHAEMIA Ischaemia or local anaemia is the local diminution of blood supply due to obstruction of inflow of arterial blood. Causes of Ischaemia
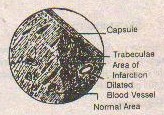
Effects of Ischaemia When the process of ischaemia is slow, there is sufficient time for collateral circulation to develop. In that case, the tissue changes are degenerative and atrophic with replacement fibrosis. Brain tissue is softened. If the cessation of blood supply is sudden and complete, the result is infarction, necrosis and gangrene. INFARCT An infarct is an area of coagulation necrosis due to complete and sudden
loss of blood supply of an organ. Collateral circulation is usually
inadequate. Infarct is termed pale when collateral circulation is minimal
(e.g., in kidney, heart and brain). When Infarct of Heart (Myocardial Infarction) The area involved includes the anterior part of the interventricular septum, the apex, and the anterior part of the wall of left ventricle. The papillary muscles are most severely affected. When the right coronary artery is occluded, the infarct includes the posterior half of the interventricular septum and posterior part of left ventricle with little involvement of the right ventricle. The right ventricle generally escapes infarction because of the collateral circulation established by the The basian vessels. Gross Appearance The areas are irregular in shape, yellow and often surrounded by a red zone. The larger areas may undergo softening leading to rupture of the heart. If the endocardial surface is involved, a mural thrombus will be formed on the necrotic area; if pericardial surface is involved, there will be patch of pericarditis. Embolism, sometimes fatal, may occur as a result of mural thrombus becoming detached. Gradually the infarct becomes replaced by fibrous tissues, so that it is represented by a white patch of scar visible both on the endocardial and on the cut surface with corresponding thinning of the wall of ventricle. If the patient survives for sometime, the weakened area will give way and buldge outward, so that aneurysm of the heart is formed with marked thinning of the wall. This usually involves the inferior wall of left ventricle near the apex. In course of time, this aneurysm may rupture causing sudden death. Microscopic Changes The changes depend upon the. age of infarct. Necrosis is evident after six hours, when the muscle fibres become hyaline and stain deep red with acid dyes. The striations are indistinct and finally lost. The spaces between the fibres are filled with granular debris and the nuclei disappear. Some of the fibres may become swollen and vacuolated before disintegrating. In the first week, there is polymorphonuclear infiltration of the necrosed area at the end of twenty-four hours. By fourth day it becomes marked. Removal of necrosed tissue begins. In the second week, this removal is carried out by great number of pigment filled macrophages which replace the polymorphonuclears. New cappillaries and fibroblasts grow into the area of infarct. In. the third week, removal of the dead muscle may Infarct of the Spleen be completed in small infarcts, though much delayed in large lesions. The fibroblasts begin to form Causes collagen. During 4-6th weeks, collagen formation is marked. By the end of second month the process is complete and the infarct is healed. Infarct of Kidney Causes
Gross Appearance The cortex is irregularly demarcated by pale, slightly depressed area, surrounded by a thin irregular margin of red, hyperaemic zone. The surface of the kidney escapes infarction besause of its blood supply from the vessels extending from capsule. The cut surface is pale, wedge-shaped with base of the wedge toward the cortex and apex toward medulla. A rim of uninvolved cortical tissue lies between the renal capsule and infarct area. Microscopic Appearance Infarct of Spleen Causes 2. Emboli arising from the heart. Characteristics 1. Red haemorrhagic; old infarcts are, however, always pale as the
haemoglobin is gradually removed. SHOCK Shock is the clinical manifestation of an inadequate volume of circulating blood accompanied by physiological adjustment of the body to the progressive discrepancy between the capacity of the vascular system and the volume of blood to fill it. Causes
Pathogenesis The sequence of events in shock is believed to be:
At first the blood pressure may be sustained (hypertensive reaction) or occasionally even raised, possibly due to diversion of blood flow from the kidneys with subsequent liberation of pressor substances. Later the blood pressure falls, owing to the Causes loss of tone in the capillaries throughout the body, with the result that blood accumulates in them and A. Cardiac: their permeability is increased so that plasma is lost into the tissues and the blood volume is further reduced. A visciOus cycle is thus established. The pressor substances causing initial hypertensive reaction are termed vasoexcitor material (VEM). This material is produced by cortex of the kidney while the kidney loses the power to destroy it. The loss of capillary tone and increased capillary permeability have been attributed to the effects of anoxaemia leading to liberation of vasodepressor material (VDM) from the fiver and muscles. The vaso-depressor material is believed to be ferritin. The vaso-excitor material and vaso-depressor material are collectively termed humoral vasotropic factors. Post-mortem Appearances The lesions are those of anoxia and increased capillary permeability:
CHRONIC VENOUS CONGESTION Causes
Changes in the Liver Gross Changes The liver becomes enlarged and tender. The cut surface shows a mottled appearance of dark brown and light yellow areas (nutmeg liver). Microscopic Changes Changes in the Lung Two forms are recognised, namely, the brown induration, a chronic process and hypostatic congestion, usually a terminal one. Brown induration is always associated with hypertension in the pulmonary
circuit. The lungs are voluminous, brown in colour, tough, and indurated.
Microscopically, the lung is filled with blood, the alveolar vessels being
widely distended and alveoli containing many red blood cells. There is
presence of large number of phagocytic cells filled with yellow pigment.
These cells are known as heart failure cells. However, it is a misnomer as
the condition is not always associated with cardiac lesion. The pigment is
haemosiderin, derived from the red blood cells.
In hypostatic congestion, the dependant part of the lung appears to be consolidated. The air in the alveoli is replaced by plasma and red blood cells, but a pneumonic process may be added as a result, of terminal infection. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||



|
Chapter 5 : Nutritional disturbances DEGENERATIONS Degeneration may be defined as the passive metabolic derangement of cells to the nonfatal injuries, which leads to different intercellular alterations, resulting in the accumulation of metabolites. Causes of Degenerations
Types of Degenerations
Cloudy Swelling It is the commonest type of degeneration caused by:
Cloudy swelling results from disturbance in prowin and water metabolism resulting in increased intracellular colloidal osmotic pressure. Mitchondria are damaged. Water is absorbed into the cells which become swollen. Commonly affected organs are kidney, fiver, adrenals and heart. The organ is slightly enlarged and looks pale. The cut surface is hazy. The cells are swollen. Cytoplasm shows albuminous granules soluble in acetic acid. Hydropic Degeneration Very large amount of water is retained by the cells resulting in marked swelling. Granules are absent in the cytoplasm. Cytoplasm is vacuolated or reticulated. Hydropic degeneration of liver is caused by poisoning due to chloroform, diethylene glycol and carbon tetrachloride. Fatty Change Fatty infiltration is caused by overload of fat and lack of lipotropic factors. It is commonly fQt*,*d in liver. The nucleus is pushed to the periphe'ry and becomes elongated and narrow. There may be individual cells or fat cysts. Amyloid Degeneration (Amyloidosis) Lipoidal Degeneration Glycogen Infiltration There is excessive accumulation of glycogen in the affected tissue. The common causes are diabetes mellitus and glycogen storage disease, an inborn error of metabolism. The common sites are kidney and suppurative lesions. Mucoid Degeneration Mucus is a loose combination of protein with mucopolysaccharides of high molecular weight. Mucous granules appear to be produced by the mitochondria, then moving to the Golgi apparatus, where they change into mucin granules. When this process is exaggerated with excessive secretion of mucus associated with degeneration of the cells, it is called mucoid degeneration. Hyaline Degeneration It is a nonspecific degeneration affecting mainly the collagenous connective tissue and fibrous tissue in the walls of the blood vessels (connective tissue hyaline). The other form is cellular hyaline. Connective tissue hyaline appears as a homogencous swelling of collagen and the walls of the vessels in arteriosclerosis. It is present in:
The cellular hyaline is seen in:
FATTY DEGENERATION AND INFILTRATION Accumulation of fat in degenerated or damaged cells is termed fatty degeneration. It is differentiated from the termfatty infiltration in which fat accumulates in apparently normal cells. However, the differentiation is an obsolete one. The two conditions are collectively termed fatty change. Pathological adiposity, having more semblance to the fatty infiltration is the term used for an increase of fat in the tissues which normally store fat. Causes
Changes in the Liver Gross Appearance Microscopic Appearance 1. Liver cells represented by large fat globules Change in the Heart Gross Appearance -Two patterns 1. In profound anaemia, there are bands of yellow coloured myocardium, alternating with bands of darker, red-brown, uninvolved myocardium. The uninvolved zones are believed to be closer to the blood vessels and are therefore less hypoxic than the yellow bands. 2. In profound hypoxic or diphtheritic myocarditis, the entire myocardium becomes flabby. Microscopic Appearance The fat in the myocardial cells tends to be distributed in minute cytoplasmic vacuoles. AMYLOIDOSIS Amyloidosis is a type of cellular degeneration in which there is deposition of amyloid in the tissue. Amyloid is a glycoprotein, the carbohydrate part being a sulphated polysaccharide and the protein part being globulin. Demonstration of Amyloid Amyloid is demonstrated by its staining reactions; the following methods are employed. 1. Iodine solution produces a dark brown colour
when poured over the cut surface of an organ. Type of Amyloidosis
Localised amyoidosis is observed in the vicinity of abscesses and the lymph nodes draining them. This is probably a direct effect of suppuration on adjacent tissue elements. However, it is the rarest form. Small connective tissue growths in the larynx, bronchi and nasal septum are sometimes composed mainly of amyloid. Amyloidosis of Spleen (Two form) A. Patchy amyloidosis Gross Appearance 2. Capsule normal. On Cut Section 1. Firm, dark red Microscopic Appearance 1. Amyloid appears in the Malpighian bodies between the
lymphocytes. B. Diffuse amyloidosis Gross Appearance On cut Section Microscopic Appearance Amyloidosis of Kidney Gross Changes 2. Firm in consistence. On Cut Section 2. Pale grey in colour. 3. Medulla may be congested. Microscopic Appearance 1. Capillary loops of glomerular tufts In advanced cases amyloid may be found lying under the epithelial cells of the tubules involving the basement membrane. Amyloidosis of Liver Cut Surface Microscopic Appearance Effects of Amyloidosis 3. In the intestines increased permeability causes watery diarrhoea. NECROSIS Death of a cell or group of cells, is termed necrosis, when such cells still form a part of the living body. Necrosis may or may not be preceded by degenerative changes. When necrosis preceded by degenerative changes, it is termed necrobiosis. Causes of Necrosis
Types of Necrosis A. Coagulation necrosis:
B. Liquefaction Necrosis: D. Fat Necrosis Changes in the Cell A. In the Cytoplasm: B. In the Nucleus: GANGRENE Gangrene is death of a part accompanied by putrefaction of the tissue by saprophytic bacteria. It occurs in organs exposed to atmosphere directly or indirectly, e.g., skin, mouth, bowel, lung, cervix, etc. Causes of Gangrene
Types of Gangrene Gas gangrene 1. Occurs in wounds inflicted in wars or in street accidents. Noma 1. Occurs occasionally in poorly nourished children especially after
some debilitating infection. Dry Gangrene Most Gangrene 1. Occurs in: 2. Owing to abundant moisture, there is rapid growth of putrefactive bacteria; the part becomes rotten, putrid, and fouls smelling. 3. Liquefaction of tissues and often gas formation, produce blebs of fluid under the skin; bubbles of gas give an emphysematous crackling when the part is palpated. 4. Local spread is rapid with no line of demarcation. 5. Toxaemia and finally death due to absorption of toxic products. ATROPHY The term atrophy refers to the acquired wasting or diminution in the size of a cell or of the essential tissue of an organ. Causes of Atrophy 2. Diminished functional activity. 3. Interference with nerve supply. 4. Continuous pressure. Defective Nutrition This may be produced locally by arterial disease interfering with blood supply to a part, when the reduction is not so severe as to cause necrosis. The functional parenchymatous elements of the tissue then undergo atrophy and there is sometimes also a concomitant overgrowth of connective tissue, the condition being called fibroid atrophy. This is often well seen in the heart wall and in the kidneys where small atrophic depressions result from narrowing of the lumina of small arteries. When the muscle cells of arterial wall are atrophied, the overgrowth of connective tissue becomes very marked. This is probably compensatory since it gives support and minimizes dilatation. General atrophy is seen in cases of starvation. Emaciation depends chiefly upon utilization of fat of the adipose tissue but there is also a great wasting of the tissues. The various organs may thus diminish in weight. The liver and spleen are markedly affected, the kidneys and heart to lesser degree whilst the central nervous system is only slightly affected. In a great majority of cases of wasting disease, however, such as malignant growth of the alimentary tract, chronic tuberculosis or suppuration, etc. a toxic element is concerned in production of wasting. Various degenerations may thus come to be associated with atrophy and secondary anaemia is present. Secondary anaemia is little marked in cases of pure starvation. The term cacharia is often applied to a condition of wasting, anaemia and weakness. Diminished Functional Activity Diminution in katabolic process leads to anabolism below the normal and thus to diminution in the size of cells. When a part is under-functioning, t e blood supply diminishes which is presumably the cause of atrophy. Accordingly it is likely that atrophy depends upon diminished metabolism. This disuse atrophy is seen when a gland, e.g., pancreas has its duct obstructed, its functional activity is stopped and it undergoes atrophy. Similarly tubules of kidney undergo atrophy when their glomeruli are thrown out of action. The muscles around a joint which has been fixed for some time undergo marked atrophy and the bones may also be affected. Interference with Nerve Supply This form of atrophy is seen where there is any destructive lesion of the lower motor neurones or their axons, the motor nerves, This type is often called neuropathic atrophy. There is not only a simple wasting but also more active degenerative changes in the nerve fibres and muscles. In the former Wallerian degeneration takes place, in which the myelin breaks down into fatty globules; whilst in the latter, fatty degeneration also occurs followed by absorption of the sarcous substance and increase of the interstitial connective tissue. Sometimes marked atrophy occurs also in the bones from the same cause, e.g., cases of infantile paralysis. The bones of the limb may become thin and light. Deficiency of the Endocrine Glands The effects of endocrine deficiency are seen mainly when it occurs at an early period of life, so that the full development of the body is interfered with and thus hypoplasia results. This is especially seen in the deficiency of thyroid and of the anterior lobe of the pituitary. A striking example of true atrophy in the adult, however, is seen in myxoedema due to thyroid deficiency. There occurs marked atrophy of the structures of the skin viz. hair follicles, sweat glands, and sebaceous glands. Continuous Pressure The continuous pressure acts mainly by interfering with the blood supply and also the functions of a tissue. Thus the pressure atrophy maybe produced by simple tumours, cysts, etc. Even bone may undergo atrophy from pressure but in this instance, there is active absorption of tissue by cellular activity, osteoclasts being concerned in the process. OEDEMA The term oedenia may be defined as an abnormal accumulation of fluid in the tissue spaces and serous cavities. This accumulation may be local or general. When water collects in the tissues, it may be in free or combined form. When combined, it may be united with the protoplasm of the tissue elements and can be moved from one place to another. Causes of 0edema
Increased Capillary Permeability Although the capillary endothelium is completely .permeable to water and crystalloids, the outward passage of colloids is closely related to the condition of the vessel wall. Under normal conditions, protein is almost completely prevented from crossing out of the blood into the tissue. But when the vessels are damaged, e.g., by toxins, anoxia, etc. they become readily permeable to proteins as seen inflammatory oedema. The escape of proteins is of greatest importance in the production of oedema, for it lowers the colloldal osmotic pressure of the blood and raises that of the tissue. As a result, water readily passes out through the capillary wall. Decreased Colloidal Osmotic Pressure of the Plasma Proteins Under normal conditions, colloidal osmotic pressure of the plasma proteins holds the water inside blood vessels and prevents it from passing into the tissues. When the level of plasma proteins becomes low resulting in decreased osmotic pressure, water passes out from the vessels into the tissues and hence oedema develops. A fall of plasma proteins below 5% will cause oedema. Thus long continued anaemia is likely to be associated with oedema. Marked ascites, when the fluid is rich in protein content as in malignant disease of the peritoneum may lead to generalised oedema (anasarca) owing to severe blood protein loss. The osmotic pressure of albumin is about four times that of globulin. Thus when there is reversal of albumin: globulin ratio (3:1) as in subacute glomerulonephritis and nephrotic syndrome, oedema sets in. The colloidal osmotic pressure, therefore depends partly upon the total amount of plasma proteins and partly upon their relative proportion. Increased Hydrostatic Pressure of Blood The pressure in the capillaries is the force which plasma and enables the normal passage of nutritive material into the tissues. If it is increased, oedema results. The pressure in the capillaries depends upon the venous blood pressure and not upon the arterial pressure. In cardiac failure the venous pressure rises markedly, and the increased capillary pressure leads to oedema. The stretching and dilatation of the capillaries also renders them more permeable. The oedema that follows thrombosis of the main vein of a limb is largely due to an increase in the capillary blood pressure. Lymphatic Obstruction This is an important factor in the production of local but not general oedema. Much of the intercellular fluid in the tissues escapes by way of the lymphatics, so that obstruction to outflow through these channels will cause local oedema. The obstruction may be due to inflammation, the presence of tumour cells within the lumen or filariasis. Pressure from outside may be due to a tumour or collection of fluid. As the fluid increases, the lymphatic obstruction becomes more marked, so that a vicious cycle is formed. Examples of lymphatic oedema are swelling of the arm in breast cancer, swelling of the legs, scrotum, etc. in elephantiasis, chylous ascites and chylothorax in thoracic duct obstruction. Milroy's disease or hereditory oedema is also probably lymphatic in origin. Chloride Retention It is a secondary factor as it does not cause the production of oedema but it aggravates and continues the already existing oedema. Once oedema is established and chlorides pass into the tissues with water, more water is retained by the tissues because of increased osmotic pressure. In renal oedema the withdrawal of salt from food is often followed by rapid disappearance of the oedema and a corresponding increase in the flow of urine. Oedema in Acute Nephritis The oedema in acute nephritis cannot be due to -protein loss in urine since the plasma proteins are normal and oedema fluid is rich in protein. The factors involved include oliguria. due to glomerular damage, and increased reabsorption of sodium and water from the renal tubules. It is probable that the subcutaneous capillaries are simultaneously damaged with those of the kidneys. A further factor is congestive heart failure with rise in capillary blood pressure. Oedema in Nephrotic Syndrome The following factors are probably concerned with the production of oedema: 1. Hypoproteinaemia. The colloidal osmotic pressure is lowered by loss of protein in the urine, and hence fluid passes from the blood into the tissue spaces. The normal colloidal osmotic pressure is 40-50 cm of water; in nephrotic syndrome it is 5-20 cm of water. The protein lost from the plasma is albumin rather than globulin owing to the smaller size of its molecule. The protein content of plasma in nephrotic syndrome does not usually fall below 4G%. A further fall in albumin figure is compensated by rise in globulin content. A second factor which may be partially responsible for the fall in albumin content of the plasma is failure to synthesize new proteins from the aminoacids. The capillary permeability does not appear to be increased in nephrotic syndrome as the oedema fluid and the ascitic fluid protein content is low. PIGMENTATION Types of Pigmentation
Endogenous Pigmentation 1. Melanin Piginentation. The melanins are ironfree sulphur containing pigment varying in colour from pale yellow to deep brown. They are formed intracellularly from colourless precursors, melanogens, by the metabolic activities of the cells and are very stable substances resistant to acids and many other reagents, but soluble in strong alkalies. They are related to the aromatic compounds, tyrosine, phenylalanine and tryptophan and may be formed from such substances by oxidation. On treating section of the skin with dihydroxyphenylalanine (dopa) certain cells in the epidermis oxidize this substance by means of an enzyme like tyrosinase and become blackened in consequence. These cells are 'dopapositive' The only cells in the skin which are dopapositive in vivo are the dendritic cells which lie extended between the basal cells of the epidermis. These cells are the only true mellanoblasts and after elaborating the pigment in the form of fine granules they transfer it by means of their processes into the basal epidermal cells and also into certain I5hagocytic cells in the dermis which may thus become heavily pigmented with coarse pigment granules. Melanin pigmentation occurs in the following conditions. (i) Addison's disease. Following destruction of the adrenal contex there occurs a general increase in pigmentation, especially in the parts exposed to light and in those normally pigmented. There may also be pigmentary deposit on the inner surface of the cheeks on a line corresponding to the junction of the teeth, and on the sides of the tongue, the position of the deposit being apparently determined by irritation. (ii) Chloasma. It is a condition sometimes due to ovarian disorder and sometimes related to pregnancy, pigmented patches occur on the skin of the face and pigmented parts, e.g., the nipples, may become of deeper tint under the influence of oestrogenic and melanocyte stimulating hormone. (iii) Leucoderma (Vitiligo) may be attended by increase in pigment
in the intervening parts. In the affected areas the dendritic cells are of
abnormal structure and have lost their capacity to oxidize 'dopa' to form
pigments. 2. Haematogenous pigmentation. Normally the breakdown of haemoglobin begins with opening of the porphyrin ring system. Iron is carried away attached to the plasma 13-globulin transferrin (siderophyllin) for preferential reutilization in blood formation. The residual biliverdin pigment is then reduced to bilirubin which is absorbed and carried by the plasma a-globulin to the liver where it is dissociated and the pigment, conjugated with glucuronic acid is excreted in the bile. In pathological states, haemoglobin is broken down in similar manner and many cells have the power to effect the change. The resulting pigments may be deposited in the tissues around some local destruction, e.g., that following a haemorrhage, or in certain organs where there has been a process of general blood destruction. When haemorrhage occurs into the tissues the red cells become haemolysed and their haemoglobin is broken down by tissue enzymes and by the action of phagocytes. The pigments usually deposited are haematoidin (iron free) and haemosiderin (iron-containing). Haematoidin is formed mainly from large accumulations of blood; thus the rhombic crystals are often met with in the sites of old cerebral haemorrhages, in thrombi, haemorrhagic infarcts, etc. It is found both in the free condition and within cells. Accumulation of haemosiderin in organs, or viseral siderosis occurs in malignant malaria and where there has been much haemorrhage into the tissue, e.g., in purpuric diseases. Malalial pigmentation. The malarial parasites within the red corpuscles produce from the haemoglobin a dark-brown pigment, haematin, in the form of very minute granules, which accumulateswithin the intracorpuscular parasites. It becomes free when the corpuscles are broken, and is taken up by phagocytes and deposited in the organs especially the spleen and liver, where it remains practically unchanged for many years. Haemochromatosis. This term is applied to a condition in which there is an extensive deposit of haemosiderin in the organs and tissues without anaemia or other evidence of increased blood destruction. It appears to be an inherited abnormality of iron metabolism leading to excessive absorption. the largest amount is present in the liver, but the haemosiderin may occur in even greater concentration in the lymph nodes in part of the abdomen. It occurs in the skin especially around the sweat glands also in the pancreas, gastric glands, heart muscles thyroid, etc. In the liver it is always accompanied by a somewhat fine cirrhosis, usually with enlargement. Biliary piginentation. This occurs especially in jaundice, the
coloration of skin and other tissues is usually due to reabsorption of bile
pigments from the liver after conjugation with glucuronic acid. The bile
pigment retained in the liver cells is deposited in the form of small
greenish brown granules, most prominently in the central parts of the
lobules. The reabsorbed bile pigment is excreted by the kidneys, and a
finely granular deposit occurs in the cells of the convoluted tubules.
Portions of the pigmented cells are broken off and form granular collections
in the tubules, and these on passing downwards become condensed, so that in
the lower parts hyaline cylinders of brownishgreen colour may be
present. Exogenous Pigmentation PATHOLOGICAL CALCIFICATION Pathological calcification may occur in normal tissue as a result of blood being flooded with calcium or it may represent the deposition of calcium in tissue which is injured, degenerated or dead. In the former case, it is known as metastatic calcification and in the latter, dystrophic calcification. Metastatic calcification may be induced by repeated injections of parathyroid hormone or it may be occur in decalcifying disease of bone such as osteoporosis of forced immobility (poliomyelitis, etc), osteomalacia, general carcinomatosis of bone and multiple myeloma. The calcium is either removed from the bones or not laid down there, but deposited in other tissues, more particularly the kidneys. Dystrophic calcification, in which calcium is laid down in dying or dead tissue irrespective of blood calcium level, in much more common. Both phosphate and carbonate are deposited in practically the same proportion as is found in the bone. There is tendency for any dying or dead tissue, accessible to the body fluids to become calcified. Necrosis and hyaline changes are the two chief antecedents of calcification. Several examples or pathological calcification are often seen, the more important being:
METAPLASIA Metaplasia is the transformation of one type of tissue into another type.
This process has definite limits. An epiblastic tissue can only produce another
epiblastic tissue, mesoblast can only produce mesoblast. Metaplasia is best
seen in the closely related connective tissues as when cartilage is converted
into bone. Thus depending upon the type of tissue involved, metaplasia may be
epithelial metaplasia, connective tissue metaplasia and endothelial
metaplasia. True epithelial metaplasia occurs in response to call for altered function or at least the result of altered environment. If the prolapsed uterus becomes everted, the columnar epithelium is changed into a stratified squamous form better suited to withstand friction. As a result of continued irritation, e.g., from gallstones, the columnar epithelium of the gallbladder may also become squamous. The more highly specialised glandular epithelia (liver, kidney, etc.) appear to be incapable of true metaplasia. Connective tissue metaplasia is of common occurence. Fibrous tissue, myxomatous tissue, cartilage and bone are all closely related and one may become changed into another. The commonest change is that of cartilage into a bone. In old age ossification of the laryngeal and tracheal cartilages is common. This is certainly not due to altered function but may be connected with the altered environment. Bone may be formed in the walls of degenerated arteries or in an eye which is destroyed and functionless. It may be encountered in the edges of a wound in the abdominal wall. In myositis ossificans bone is formed in the voluntary muscles and may replace them to a large extent. The cells of an osteogenic: sarcoma of bone may form fibrous tissue, mucoid tissue, cartilage or bone. Endothelial metaplasia is observed when serosal endothelium as that lining the pleura or peritoneum is irritated. In place of being flattended it may become cubical, columnar or even startified. The cubical and columnar cells may surround spaces so as to give glandular appearance. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||


|
Chapter 6 : Granulomata INTRODUCTION A granuloma is a variety of chronic inflammation characterised by lesions which tend to be strictly circumscribed and by cells of histiocytic rather than of haematogenous type. A granuloma is essentially a highly specific reaction of the reticuloendothelial system. Thus the granuloma must be regarded as a special example of inflammation and not as a tumour since the latter should have no relationship with the reaction to iinjury or limitation of infection.
TUBERCULOSIS Tuberculosis is caused by the acid fast organism, Mycobacterium tuberculosis. Two types - human and bovine, are known to cause infection in human beings. Both types are equally pathogenic for man. The bovine bacillus is primarily a parasite of cattle. In man it is mainly responsible for tuberculosis of lymph nodes and bones in children. Infection with the human type is air-borne from patients with pulmonary tuberculosis (i.e., with viable bacilli in the sputum). Infection is commonest under five years of age when it is likely to be rapidly progressive and fatal. Then it declines until late adolescence, reaching its maximum in women between 20-25 and in men between 40-50 years of age. In the adult the disease is much more chronic. Infection may occur through the alimentary tract by ingestion of infected milk especially in the rural population where proper boiling is not practised. Congenital infection through the placenta is rare. Spread The tubercle bacillus is non-motile but it can be transported in the bodies of phagocytes. The spread may occur by:
Spread by direct extension occurs from the primary site of lesion. The extension is effected by amoeboid movement of the phagocytes harbouring the bacilli. Thus the bacilli are carried into the lymph spaces of the surrounding tissue. Spread by lymphatics results in transportation of the bacilli from the infected lymph spaces to the regional lymph nodes whence they disseminate widely in the lymphatic system. Ultimately the bacilli are poured into the venous blood stream through the thoracic duct. The venus blood carries the bacilli to lungs and sometimes to systemic circulation. Spread by blood stream may occur either via the lymphatic-venous route or by ulceration of a caseous focus into a vein. In the former case, a simple bacillaemia results leading to isolated lesion in almost any organ of the body. While ulceration of a caseous focus into a vein results in general miliary tuberculosis and the circulation is flooded with bacilli; tiny miliary tubercles, macroscopic or microscopic are present in every organ of the body. Spread along the natural passages may occur through the bronchi, ureters
and vas deferens. In these cases however, it is difficult to be certain that
the bacilli have not been carried along the lymphatics in the
submucosa.
Primary Tuberculosis (Ghon Lesion) Gross Appearance 2. 1 - 1.5 cm in diameter. 3. Grey-white inflammatory consolidation with sharp boundary. Microscopic Appearance 1. At very early stage centre of focus consists of a collection of swollen
macrophages around which there is a zone of round cells, chiefly
lymphocytes.
2. Soon macrophages become oval, spindleshaped, or irregular in form, w4h fairly abundant cytoplasm and a faintly staining nucleus. These cells are termed epithelioid or endothelioid cells. 3. The central cells become swollen and lose their outline, their nuclei cease to stain and ultimately they become fused to become a homogeneous or slightly granular, structureless material (caseation necrosis). 4. Among the epithelioid cells are the giant cells with some what irregular outline and numerous oval or rounded nuclei often arranged at the periphery (Langerhan's giant cells). The primary tubercle or primary complex or Ghon lesion has thus a necrotic centre surrounded by epithelioid cells with a few giant cells and these again surrounded by small round cells. LEPROSY Leprosy is a chronic infective granuloma caused by Alycobacterium leprae,
an acid-fast bacillus, chiefly affecting the skin and nerves.
This form is manifested especially in the skin by diffuse involvement in which the skin becomes erythematous, swollen and often smooth and glistening. It is firm and usually painless. Projecting nodules may develop, either discrete or fusing to form large conglomerate masses. When the latter involve forehead and face together with loss of eye brows and eye lashes, the face is discribed as leonine. Involvement of conjunctivae leads to blindness; hearing, smell and taste sensations are sometimes lost. The nodules vary in size from microscopic to 2 cm. diameter. The large nodules, often in the skin, are well defined, have a tense overlying epiderm, are firm, somewhat elastic and cut with resistance. They show a slight buldging; pale yellow or light grey in cross section. Situated in the corium, they may extend deeply. Microscopically, the nodule is made up principally of large, mononuclear cells, with an irregular intermingling of lymphocytes, plasma cells and multinucleate giant cells of Langerhan's type. The large mononuclears and giant cells are often foamy and contain the acid fast bacilli. These foam cells may also contain fat. The bacteria may also be found in vascular endothelium, in polymorphonuclear leucocytes and even in epithelium. They are present as small clusters of organisms termed. 'Cigar pack' and as large masses. Extracellular organisms are also found but these are originally intracellular. Occasionally, lepromas are made up largely of large mononuclear cells without foamy cytoplasm. Sometimes there is an ingrowth of connective fissue and the losion becomes cicaterized. Tuberculoid Leprosy Tuberculoid lesions are tiny granulomas, often near blood vessels, made up of lymphocytes, large mononulears, and occasional giant cells. When in the skin they are in the upper corium, and the overlying epidermis is often atrophic. The lesions are smaller than the usual leproma and also differ in that they contain few demonstrable bacteria. Sometimes tuberculoid lesions, especially in the lym- ph nodes and bones, closely resemble the granulomas of sarcoidosis. In rare instances, tuberculoid lesions undergo extensive necrosis with the formation of painless ulcers, called lazarine leprosy. Indeterminate Leprosy The lesions are not distinctive histologically. Hyperaemia is prominent in the erythematous macules. Infiltration of lymphocytes may be noteworthy, especially around blood vessels. Dimorphic Leprosy The histology is not characteristic. As changes occur, the lepromatous or tuberculoid features may be prominent. SYPHILIS Syphilis is a specific infective granuloma caused by Treponetnapallidum and transmitted sexually. The lesions encountered in syphilis are described in three stages viz. primary, secondary and tertiary. 1. Primary lesion. The primary lesion appears at the site of incoulation. This is usually on the genitalia but it may be extragenital, e.g., on lips and fingers. The common genital sites are the penis in the male and the cervix in the female. The cervical chancre is highly infective on account of the moist character of its surroundings and it is easily overlooked owing to its hidden nature and freedom from pain and discharge. The primary lesion is generally single but may be multiple. It usually develops in from three to fourweeks after infection but this latent period may be two to six weeks. It f irst takes the form of a hard nodule but the surface tends to become ulcerated and a 'hard sore' or chancre is formed from the surface of which enornious number of spirochactes are discharged. The chancre is the earliest clinical manifestation but from the pathological standpoint the chancre is really a late affair. The hardness is due to dense cellular infiltration but does not appear during the first few days. Later it is caused by a marked degree of fibroplasia. In the course of a few weeks, healing occurs which may or may not leave a scar. Microscopically, there is dense accumulation of lymphocytes and plasma cells especially around the small vessels and fibroblasts multiply and lay down collagen fibrils. Destruction of the tissue is seldom marked but the surface epithelium is usually lost. The regional lymph nodes are enlarged, hard and shotty but not painful or tender. 2. Secondary lesion. After the appearance of primary lesion, there is a latent period. In two or three months after infection, secondary lesions appear in the skin, mucous membranes and the central nervous system. These persist for a period of months and then disappear. There is no destruction of the tissue at this stage so that no scars are left. Secondary lymphadenitis is one of the earliest changes. Swelling of the epitrochlear or posterior cervical nodes are specially characteristic. The lesions of the skin are of great variety, but they are symmetrical in distribution. They are polymorphous in type, i.e., present several varieties of the lesions at the same time. The lesions may be macular, papular or pustular. 3. Tertiary lesions. The subsidence of the secondary lesions is followed by another latent interval during which all is quiet. In a year or not for many years a third set of lesions appears. These are not symmetrical. They affect deep as well as superficial structures and show a tendency to necrosis and destruction. These are not infective. Two main types of tertiary lesions may occur. The one is gross and localised (the gumma), the other is microscopic and diffuse. The gumma is a necrotic, localised, yellowish, homogeneous mass of rubbery consistence composed of usual mononuclear cells. In the centre of the lesion necrosis and caseation occur with the formation of peculiar gummy material, but there is not the same complete wiping out of structure as in tuberculous caseation. A few giant cells may be seen at the margin. Gummata of skin, mouth, tongue and nose may lead to extensive ulceration. The liver may show one or several masses which heal with fibrosis so that deep scars are formed producing a peculiar lobed appearance known as 'Hepar lobatum'. In the testicle, gumma forms a hard mass which may be confused with tumour. Gumma in the bone, the brain and other places may be confused with tumours of these organs. In the diffuse lesions, the spirochaetes are widely distributed and set up a diffuse chronic inflammatory reaction which lymphocytes and plasma cells, tissue destruction but no caseation. The principal sites are the thoracic aorta and the testicle. In the thoracic aorta a frequent result is the development of an aneurysm of that vessel. The most serious of all the late lesions are those of the central nervous system which may appear many years after the original infection., These may affect chiefly the meninges, the brain and the spinal cord. Congenital Syphilis Syphilis may be transmitted from the father or mother but in all cases mother is infected though the infection may not be manifest. There are three possibilities: 1. The child may be born dead showing well marked evidence of
syphilis. When the child is born dead, the appearance is usually characteristic.
There is no primary lesion, as infection takes place through the placenta.
The child is usually premature and undersized. The skin may be macerated. The
spleen and often the liver are enlarged. Syphilitic epiphysis is the most
diagnostic feature. The chief microscopic change is an interstitial round
cell infiltration of many of the internal organs combined with a varying
degree of fibrosis. In the liver this produces a fine form of intercellular
cirrhosis. In the late type, lesions develop over a period of years. The permanent teeth show the appearance known as "Hutchinson teeth". These are small, widely spaced, peg-shaped and central incisors are notched: molars are pitted and honey-combed. An interstitial keratitis develops as the time of puberty producing a ground-glass opacity in the cornea. Nerve deafness is common. There may be involvement of the central nervous system similar to that seen in the acquired form. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

|
Chapter 7 : Tumours INTRODUCTION A tumour or neoplasm is a purposeless growth that progresses without
regard to the surrounding tissues or the requirement of the organism as a
whole. Whilst forming a part of the body, a tumour and its cells seem to have
escaped from the normal controlling influences of the body. Autonomy may be
regarded as the most characteristic feature of a tumour. It behaves like
a Types of Tumours
CAUSATION OF TUMOURS Causation of tumours is an intricate question and not finally decided. It appears that two factors are responsible, an initiating agent and a promoting agent. The initiating agent starts the process while the promoting agent carries it on to maturity. The initiating agent is believed to produce an instantaneous change in the cell, a somatic mutation, which however, does not manifest itself as neoplasia until the long continued action of the promoting agent renders the condition irreversible. Urethane, when applied to the skin of the mouse will not produce an evident neoplasia, but when this is followed by the repea*LC.d application of croton oil a neoplasm jcvclops. I he croton oil is harmless unless the process has initiated by urethane, for it only promotes the proce-,s. The known factors causing tumours are enlisted below:
Fig 7. 1: Sequential stages in Chemical carcinogenesis (left) in evolution of cancer (right) SPREAD OF TUMOURS The tumours may spread by the following methods:
1. Spread by infiltration. Spread of cancer cells through tissue spaces is one of the chief characteristics of malignant tumour. Cancer cells are amoeboid and motile. The cells of benign tumours and of normal tissues are incapable of movement because they are firmly anchored to one another by cell adhesiveness. Loss of adhesiveness in cancer cells is due to deficiency of calcium in the cell membrane. 2. Lymphatic spread. The tumour cells can readily enter lymphatic
channels. They may extend along
3. Spread by blood. Cancer cells may reach the blood either by way of the thoracic duct or by direct invasion of the blood vessels. The veins are invaded with great readiness but the arteries very rarely. Clumps of tumour cells may form emboli but they may not give rise to metastases owing to inability to become colonized at the site of impaction. Three groups of veins are chiefly invaded: (i) The portal system of veins is invaded by turnours of gastrointestinal
tract and pancreas. Secondary tumours of the liver are, therefore, very
common. 4. Spread by natural pagsages. Tumour cell may be carried along such passages as the bronchus, bowel and ureter. This explains the simultaneous occurrence of the same type of tumour in the renal pelvis and the bladder. 5. Spread through the serous cavities. The method known as
transcoelomic spread is the explanation given for the frequent transfer of
tumour cells from the stomach to the ovaries; small implatations on the
peritoneum can often be traced between stomach and ovary. Malignant glial
tumours shed cells into the ventricles and subarachnoid space, throughout
which they may be carried by the cerebrospinal fluid and form m ultiple
secondary growths. MALIGNANT TUMOURS Three characteristics of malignancy are: In addition the malignant tumours have the following features. However, the presence of all the features is not essential in a particular tumour: 1. Recurrence 4. Loss of polarity. Normally the epithelial cells are arranged with their
long axes perpendicular to the surface of the sheet. In malignancy there is
loss of normal polarity so that the cells now present a jumbled arrangement
to the surface.
Types of Carcinoma
Glandular Carcinoma The growth may take origin from the acini of the glands or epithelium covering mucous surfaces or lining ducts. Spheroidal-cell carcinoma is the term applied when the cells are rounded or polyhedral in form and adhere together to form solid masses of various sizes. This is the most atypical form and the cells show no attempt to produce a gland like arrangement. In adenocarcinoma, the cells are more cubical or columnar and tend to form a more or less complete lining of the alveoli in which they lie. Thus, they produce, though imperfectly, a glandular structure. The lining of the alveoli may be fairly regular in places, but usually there is evidence of excessive proliferation in the irregular folding and heaping up of the epithelial layer. The cancer cells may, at places, form papilliform processes (e.g., in lung and thyroid) or trabeculae (e.g., in liver).
Fig 7.3 : Adenocarcinoma of Cancer Adenocarcinorna is termed scirrhous when tl~.. mass is compact to give hard consistence. It is termed encephaloid when it forms a soft fungating mass. Mucoid Carcinoma It is essentially carcinoma in which the cells form much mucin and then disintegrate to become fused with the mucoid material, no cells surviving. Such tumours are commonest in situations with abundant mucin forming cells, notably in the large intestine, biliary passages, stomach etc. The tissue of the tumour has a characteristic semitranslucent appearance; at places it may be softened and glue like. A constant feature is the formation of a large mass Extension to the distant lymph nodes is prevented by blockage of the lymphatics which mucoid material. Squamous Carcinoma It is derived from the stratified squamous epithelium of the skin or of a mucous membrane, or form an epithelium which has undergone metaplasia into the squamous type, e.g., in bronchi, gall bladder, renal pelvis etc, It may also arise from the cellular inclusions of congenital origin, e.g., from bronchial clefts, dermoid cysts etc. Naked eye appearance. A squamous carcinoma appears first as indurated thickening of the skin epithelium or mucous membrane. Its growth is usually slow and margins badly defined. Ulceration generally occurs at an early stage and then the esion appears as a progressive ulcer with irregular nd indurated floor and margins. Continuous growth and ulceration go on until ultimately there may be extensive destruction of tissue, Haemorrhage from erosion or vessels is of common occurrence and occassionally a fatal result is produced by the implication of a large artery. Microscopic appearance. Squamous carcinoma begins as a thickening of the epithelial layers and downgrowth of the interpapillary processes. Such changes are common at the margin of any chronic ulcer and it is often difficult to say whether or not malignancy has supervened. After a time however, the epithelium penetrates deeply as branching processes which involve the tissue spaces and destroy intervening structures such as muscle. For a time cells form a continuous mass and the shape of the growth may be compared to an inverted cauliflower. Later, however, the cells become detached and wander in tissue spaces and into the lymphatics; they are thus carried to lymph nodes, where they produce secondary growths. Metastases may occur in internal organs but are rarer than in the case of glandular carcinoma. The deepest layer of the original epithelium is continuous with the epithelium on the outer aspect of the cell masses of tumour, while the superficial or squamous layer is continuous with the central parts of the tumour cell masses. Accordingly the cells towards the centre become somewhat flattened and concentrically arranged and ultimately undergo keratinization. Such concentric structures are common in well differentiated squamous carcinomata and are known as cell nests. These cell nests are prominent in squamous carcinomata of 'skin and tongue in certain situations, e.g., in the extrinsic tumours of the larynx and in the cervix uteri, these maybe almost absent. The centre of the cell nests may occassionally show a hyaline change as in tongue. Sometimes the cell nests may be invaded by polymorphonuclear leucocytes. Basal Cell Carcinoma It is one of the commonest malignant tumours. It originates from the epidermis, chiefly in the face. Although it arises from the same epithelium as does the squamous carcinoma, it is very different tumour. It takes origin by downgrowths from the under surface of basal fayer. It is usually slow growing and spreads laterally rather than deeply. Much of the central area is lost by ulceration but the growing invasive edge of the tumour gives rise to the characteristic rolled edge. Its most remarkable feature is the extreme rarity of metastasis. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||



|
Chapter 8 : Cardiovascular system RHEUMATIC FEVER Etiology Pathogenesis Sites of Lesion
Pathology
Laboratory Diagnosis
Jone's Criteria
RHEUMATIC HEART DISEASE Rheumatic fever affects all the three layers of heart viz pericardium, myocardium and endocardium. (pancarditis) Spread of Infection Gross Appearance Mac Callum patch. Rough, thickened patch on the posterior wall of the left auricle just above the mitral valve. Microscopic Appearance 1. Neovascularization. Proliferation of blood vessels Myocardial Lesions Microscopic Appearance
Subacute Stage Pericardial Lesions (Acute Pericarditis) Gross Appearance Microscopic Appearance Aortic Lesions Microscopic Appearance 1. Intima comprises cellular, vascular connective tissue. BACTERIAL ENDOCARDITIS Classification
SUBACUTE BACTERIAL ENDOCARDITIS Course. 6 weeks to several months Etiology. Infection occurs on previously damaged heart. Predisposing Factors 1. Rheumatic lesion 75-95% cases Causative Organisms Streptococcus viridans (95% cases) Pathogenesis 1. Alterations in blood flow which induce jet effects and zones of
turbulence with low pressure pockets. Pathology 1. Mitral valve is most often involved, aortic valve is involved
less frequently. Sequelae 1. Fragmentation and embolism of vegetations may lead to myocardial
infarction Laboratory Findings 1. Progressive microcytic hypochromic anaemia 2. Leucocyte count usually normal with raised polymorphs 3. Blood culture may reveal causative organism 4. Complement-fixation reactions, specific for causative organism 5. Rheumatoid factor present in later stages, in about half the patients. ACUTE BACTERIAL ENDOCARDITIS Etiology 1. Occurs most commonly in previously normal hearts. 2. The commonest causative organism is Staphylococcus aureus. Pneumococcus and Streptococcus pyogenes are infrequently involved. Pathology Other changes and sequelae are same as in subacute bacterial endocarditis. MYOCARDIAL INFARCTION Causes of Coronary Occlusion 1. Atherosclerotic narrowing of coronary artery: 2. Haemorrhage into an atheromatous plaque resulting in: 3. Organization of a thrombus. Gross Appearance 1. The area involved includes: 2. The infareted area is irregular in shape, yellow, and often surrounded by a red zone. 3. The larger areas may undergo softening leading to rupture of the heart. 4. If the endocardial surface is involved, a mural thrombus will be formed on the necrotic area; if pericardial surface is involved, there will be a patch of pericarditis. 5. Embolism, sometimes fatal, may occur as a result of mural thrombus becoming detached. 6. Gradually infarct becomes replaced by the fibrous tissue, so that it is represented by a white patch of scar visible both on the endocardial and on the cut surface with corresponding thinning of the wall of ventricle. Microscopic Appearance 1-6 hours 6-24 hours 1- 7 days 1-6 weeks Fibrovascular tissue entirely replaces the area of necrosis; in large
infarcts this process may take several months,
B. Biochemical Changes HEART IN HYPERTENSION Gross Appearapce Compensated Stage Decompensated Stage Microscopic Appearance 2. Nuclei often elongated; some assume bizarre shape. CONGENITAL HEART DISEASE Classification
Patent Ductus Arteriosus 1. Twice more common in females Atrial Septal Defects 1. Commonest and least important congenital cardiac
abnormality Lutenbacher's Disease Combination of atrial septal defect with mitral stenosis (congenital or rheumatic). Unlike in isolated mitral stenosis, left atrium is not dilated as the blood passes into the right atrium. Ventricular Septal Defect (Rogers' Disease) 1. Right ventricular hypertrophy, dilatation and failure
Coarctation of Aorta Infantile Type 1. Constriction proximal to ductus, between ductus and subclavian
artery Adult Type 1. The constriction is at or just distal to the ductus, which is
obliterated Ebstein's Disease 1. Downward displacement of the tricuspid valve Malformation of Aortic Bulb 1. Septum of aortic bulb is pushed to the right Tetrology of Fallot Eisenmenger's Complex Tranposition of Great Vesseis 1. Results from failure of normal spiral twisting in aortic bulb. 2. Pulmonary artery arises from left ventricle, aorta arises from right ventricle. 3. Condition is incompatible with extrauterine life but may be compensated
for a time by: Truncus Arteriosus 1. Aorta and pulmonary artery arise from a common stem vessel, truncus arteriosus. 2. Truncus arises from both the ventricles, overriding a ventricular septal defect; interventric~ilar septum may occasionally be absent. 3. Atrial septal defect commonly present. Tricuspid Atresia 1. Right ventricle under-developed; absent in extreme
cases. Aortic Atresia 1. Aortic orifice hypoplastic Pulmonary Stenosis 1. Stenosis of pulmonary valve Anomalies of Venous Return 1. Superior vena cava or inferior vena cava or both may open into
left atrium. ARTERIOSCLEROSIS Types of Arteriosclerosis 1. Atherosclerosis (Atheroma) ATHEROSCLEROSIS Etiology
Pathogenesis 1. Imbibition of lipids. Results from lipaemia caused by high fat content
of the food. High blood cholesterol level predisposes to atherosclerosis in
cases of. 2. Changes in the vessel wall. Such changes may determine localisation of lesion. Degeneration of the mucopolysachharides of ground substance of intima may lead to deposition of lipids. Capillary haemorrhage resulting from vascularisation of the lesion provides an abundant supply of lipids. 3. Thrombosis. Thrombotic incrustations of the intima occur with material derived from the blood, the platelets in early stages and the fibrin deposits later. The lesions are superficial to begin with but later become incorporated in the intima.
Gross Appearance 1. The most severe changes are seen in aorta, particularly the abdominal aorta; more marked in descending than ascending aorta; also marked around mouths of intercostal and lumbar arteries. 2. Initially, fatty degeneration of intima in the form of irregular yellowish patches or streaks often arranged in a longitudinal direction; occasionally erosion of surface may occur. 3. Later, these patches become distinctly raised, increase in extent, thickness and become confluent. 4. if a well formed patch is incised, yellowish pultaccous material is found in deeper part of intima, next to media, being separated from the lumen by connective tissue layer, at times thick making the patch firm and of wheatish colour on surface view. 5. At a later stage, the covering of the patch may give way and the pultaceous material may be discharged into the blood stream; an atheromatous ulcer is thus formed. 6. The affected aorta undergoes dilatation and occasionally aneurysm follows: Microscopic Appearance J. Sudanophilic lipid accumulates in the stellate cells of intima, in
macrophages, and endothelial cells. Effects Monckeberg's Sclerosis Affects mainly the vessels of the limbs; exampla,, are pipestem radials and tortuous, prominent temporals. It is a senile degenerative condition unrelated to hypertension. Gross Appearance 1. Fatty degeneration of media Microscopic Appearance 1. The muscle fibres undergo fatty change with degeneration, fragmentation
and deposition of lime salts, which may be in the form of fine granules or
large masses. Rarely bone with bone marrow may be detected.
2. other coats are often normal; atheroma is often associated producing marked occlusion as seen in senile and diabetic gangrene of leg. Diffuse Hyperplastic Sclerosis Generalised hypertrophy of arterial wall with subsequent fibrous replacement; caused by hypertension; also termed arreriolosclerosis. GrossAppearance 1. The arterial wall is firmer and thicker Microscopic Appearance 1. Hypertrophy and hyperplasia of the circular muscle fibres of media and
longitudinal muscle fibres of the intima next to internal elastic
lamina. ANEURYSMS An aneurysm is a space or sac formed by the widening or extension of the lumen of an artery and containing blood or clot. Classification
Syphilitic Aneurysm Etiology
3. Commonest sites are: Effects 1. Pressure on surrounding structures leads to syndrome of superior
mediastinal compression; the great veins may be displaced and undergo
thrombosis resulting in congestion of the head and neck, and opening of
collateral channels. Atheromatous Aneurysm Etiology 1. Occurs after 50 years of age. Effects 2. Thrombosis of aorta or its branches producing ischaemia of legs, kidneys, etc. 3. Pressure effects not marked. Dissecting Aneurysm 1. Commonest after 50 years of age. Effects 1. In rupture shortly above the aortic cusps, blood commonly passes backwards and within a few hours enters the pericardial sac causing death. Intrapericardial rupture may be preceded by signs of coronary occlusion from pressure upon these vessels at their origin. 2. In rupture distal to ductus arteriosus, the blood may flow through a new channel from the aperture of entry to the point of re-entry in the lower abdominal aorta when the patient survives for some time. Occasionally a dissecting aneurysm may remain localised. Infective Aneurysm Etiology Effects Cerebral Aneurysm Etiology 1. Common site is circle of Willis and its branches Effects 1. Subarachnoid haemorrhage Traumatic Aneurysm Caused by injury to the vessel wall by a stab or bullet wound, or by spicule of fractured bone. Racemose Aneurysm 1. A form of arteriovenous fistula. 2. Appears as a pulsatile swelling consisting of Causative organisms.
Pyogenic bacteria, syphilis, tortuous and dilated arteries and veins in
tuberculosis, viruses, fungi, parasites. intercommunication. 4. Results from contusion of scalp; sometimes congenital. ARTERITIS Etiology
INFECTIOUS ARTERITIS Causative organisms. Pyogenic bacteria, syphilis, tuberculosis, viruses, fungi, parasites. Modes of Infection A. Direct invasion from: B. Haematogenous spread. Infective endaortitis results from bacterial endocarditis or septicaemia. Pathology POLYARTERITIS NODOSA Etiology 1. Collagen disease caused by hypersensitivity. Gross Appearance 1. Mainly affects arteries of gastrointestinal tract, kidney and
heart. However, brain, lung and skin may also be affected. Microscopic Appearance 1. Increased permeability of the vessel wall.
Effects
TEMPORAL ARTERITIS 1. Chronic inflammatory process involving temporal arteries of elderly
persons, extending to arteries of scalp and face. Gross Appearance 1. In addition to temporal arteries, the lesions are also present in aorta, radial, subclavian, femoral, coronary, renal, mesenteric and retinal arteries. 2. The vessel can.be felt as cord like swelling. Microscopic Appearance 1. Inflammation spreads from adventitia to media. AORTIC ARCH SYNDROME Etiology 1. Predominantly a disease of young women in the reproductive years
(young female arteritis). Gross Appearance 1. Thickening of the wall of arch of aorta and of the origin of main
vessels arising from it. Microscopic Appearance Same as in temporal (giant cell) arteritis; hence also called giant cell aortitis. ENDARTERITIS OBLITERANS Etiology 1. Atherosclerosis involving the muscular arteries of lower extremities,
with associated thrombosis. Pathology 1. Obliteration or narrowing of arterial lumen due to formation of a mass of well vascularised concentric laminae of cellular connective tissue in intima.
2. New elastic tissue is laid down independently of internal elastic lamina and may appear as a layer under the endothelium or as a number of small new laminae at various points in the intima. CARDIOVASCULAR SYPHILIS Types of Syphilitic Lesions 1. Lesions in the heart 2. Lesions in the arteries (i) Endarteritis (ii) Mesaortitis (iii) Aneurysm. Lesions in the Heart Incompetence of the aortic valve is the commonest form and is due to involvement of cusps or the valve ring. The cusps are elongated and pendulous but do not become adherent or calcify. The mitral valve is not affected but secondary incompetence may result from left ventricular dilatation. Myocardial ischaemia may follow narrowing of the orifices of the coronary arteries by intimal fibrous plaques formed over areas of mesaortitis or by cicatericial contraction of healing lesions. This results in diffuse myocardial fibrosis and angina pectoris, but myocardial infarction is rare. Death is oftensudden. Gumma of the heart is very rare. It forms a tumour like mass in the wall of a ventricle or in the interatrial septum where it may cause heart block. It is found in both congenital and acquired forms of the disease. Interstitial inyocarditis occurs in congenital syphilis and
spirochaetes are often numerous occurring in clumps throughout the cardiac
muscle. There is variable amount of fibrous tissue proliferation around
them. Lesions in Arteries Syphilitic endarteritis and periarteritis occur in small arteries. There is intimal and adventitial fibrosis associated with infiltration of lymphocytes and plasma cells around them. These changes are due to presence of treponemata in the adventitia. In some cases the change is diffuse and a number of vessels show general thickening, while in others it is of a patchy or nodular type. Syphilitic Aortitis Gross Appearance Microscopic Appearance
TUMOURS The tumours arising from the blood vessels are: 1. Haemangioma 1. Haemangioma It is of two types: 2. Sclerosing Haemangioma The capillaries become partially or completely obliterated, while only segregated groups of endothelial cells remain. It may be difficult or impossible to determine the vascular origin of such a lesion. Microscopically three different elements may be present in varying
proportion: The histiocytes may fuse to form foreign body giant cells. Both haemosiderin and the lipid may be presumed to be the result of haemorrhage from capillaries undergoing destruction. 3. Haemangio-endothelioma It is a true neoplasm of the vascular endothelium. It may be benign or malignant. Benign haemangio-endothelioma occurs chiefly in the skin but may occasionally be found in the viscera, especially the liver and spleen. It forms well circumscribed firm mass, a few centimetres in diameter and reddish grey in colour. Microscopically it consists of masses and sheets of spindle shaped endothelial cells, uniform in size and appearance, with large vascular spaces surrounded by these masses of cells. Malignant haemangio-endotlielioma, also called haemangio-endotheliosarcoma, may occur anywhere in the body. It forms a large, pale, soft mass with ill defined margins, and frequent central areas of necrotic softening and haemorrhage. Microscopically it shows the familiar malignant picture of cellular pleomorphism, anaplasia and numerous mitoses. The tumour is locally invasive and spread takes place by the blood stream, with the formation of distant metastases. 4. Haemangiopericytoma In this tumour, the cells, derived from pericytes, lie outside the vascular sheath and are closely packed about the numerous capillary sized vessels which are lined by normal endothelium. The neoplastic pericytes usually resemble epithelium, but it they become spindle shaped, haemangiopericytoma may easily be mistaken for a vascular fibrosarcoma or leiomyosarcoma. The tumour occurs most often in the extremities and is slow growing and painless. 5. Kaposi's Sascoma This very rare lesion is also known as idiopathic multiple haemorrhagic sarcoma. Multiple bluish. red patches occur in the skin and occasionally in viscera. the disease is of long duration. At first the skin lesions may resemble capillary haemangiomas but in the course of time, they become cellular, neoplastic and invasive. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||




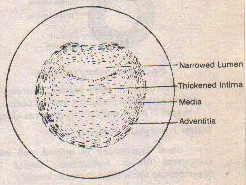
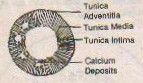



|
Chapter 9 : Urinary system ACUTE GLOMERULONEPHRITIS Etiology 1. Secondary to infection in some site of the body; commonest cause is
haemolytic streptococcal infection of the respiratory tract, other organisms
may be pneumococcus, or Streptococcus viridans. Gross Appearance Cut Surface Microscopic Appearance Tubular Lesions 1. Retrogressive changes in tubular epithelium, affecting
particularly that of proximal convoluted tubules. 2. Desquamative nephritis. Excessive desquamation of the degenerated and
necrotic epithelium. Glomerular Lesions Glomerular lesions may of three types. A. Acute degenerative glomerulitis 1. Blood in the subcapsular space and adjacent tubules; resulting from
deterioration of the cells of capillary loops. B. Acute exudative glomerulitis C. Acute proliferative glomerulitis Most common type may be of two forms: 1. Intracapillary form: The entire tuft is considerably enlarged and occupies the entire capsular space. The capillary loose are free of blood, due to swelling and proliferation of the capillary endothelium. Occasionally, a few polymorphs may be observed in the capillary loops and interstitial connective tissue. 2. Extracapillary or subcapsular form: Swelling or proliferation of the epithelium underlying the capsule of Bowman. The mass of cells may form a circular rim around the glomeruli or a crescentic mass. SUBACUTE GLOMERULONEPHRITIS Gross Appearance 1. Enlarged, slightly or considerably Cut Surface 1. Marked swelling and pallor of the cortex Microscopic Appeamnce 1. Glomeruli enlarged 3-4 times; without blood.
4. Degenerative changes in the tubules due to lack of blood supply to
medullary portion. CHRONIC GLOMERULONEPHRITIS
Microscopic Appearance 1. Renal archetecture completely lost. PYELONEPHRITIS Etiology Causative Organisms
Modes of Infection 1. Ascent from below in: 2. Haematogenous. Predisposing Factors 1. Diabetes mellitus Gross Appearance The lesions may be local or diffuse. The changes vary with the stage of the disease. A. In acute stage Cut Surface
HYDRONEPHROSIS Causes of Hydronephrosis
Gross Appearance 1. Pelvis and calyces are greatly dilated. Hydronephrotic fluid is relatively sterile as continuous circulation is
maintained by: Microscopic Appearance 1. Initially only tubular atrophy; glomeruli normal. Complications 1. Hypertension ARTERIOLAR NEPHROSCLEROSIS Types of Nephrosclerosis 1. Benign hypertensive nephroscierosis Benign Hypertensive Nephrosclerosis Gross Appearance On Cut Section Microscopic Appearance Malignant Hypertensive Nephrosclerosis Gross Appearance On Cut Section Microscopic Appearance 1. Patches of interstitial change (cellular and fibrotic). Senile Nephrosclerosis Gross Appearance Microscopic Appearance Causes of Contracted Granular Kidney
Gross Appearance Microscopic Appearance Haemosiderosis and Haemoglobinuric Nephrosis RENAL SYPHILIS Syphilitic Lesions in the Kidney
Congenital Interstitial Nephritis The kidney of congenital syphilis is characterised by interstitial inflammation in association with great numbers of treponemas in the interstitial spaces, in the tubular lumen and among the tubular epithelial cells. Gumma Syphilitic Nephrosis 1. Manifests as sudden onset of nephrotic syndrome, without renal
insufficiency. Syphilitic Focal Interstitial Nephritis Asymptomatic damage to the kidney in secondary stage of syphilis. RENAL CALCULI Structure of Renal Calculi The calculus consists of a nucleus of organic matter around which urinary
salts are deposited in concentric layers which are bound together by a
colloid matrix of organic matter. The salts, although crystalline in the
urine, are in the form of amorphous granules in the calculus. The calculi may
consist of. Mode of Formation 1. Infection. Infection is important in the secondary phosphate stone which is a common consequence of cystitis associated with enlargement of the prostate. It is probable that a mild infection is the starting point of all the uric acid and oxalate stones in the kidney, although, it is not readily detected like the gross infection which is responsible for the secondary phosphate stones. The type of the stone depends upon the reaction of the urine and that depends upon infection. A uric acid or oxalate stone is formed when the urine is acidic. Infection with pyogenic cocci turns the urine alkaline and the stone becomes coated with phosphate. Subsequent infection with Esch. coli may bring back an acidic reaction with deposition of uric acid or calcium oxalate. 2. Concentration of the crystalline salts. The relation of colloids of the urine to the crystalloids is probably of great importance. The presence of an abnormal colloid or absence of a normal one may cause crystalloids to be precipitated, especially if they are present in excess. 3. Parathyoid tumour. This is commonly associated with bilateral and recurring calculi. As a result of hyper-parathyroidism, calcium is removed from the bones, the blood is flooded with calcium and this tends to be deposited in the renal pelvis. Such stones have high content of calcium and phosphates. 4. Vitamin A deficiency. Lack of this vitamin leads to keratinization and desquamation of the epithelium of the renal pelvis which may form the nidus for a stone. It also affects the urinary colloids so that they fail to hold the crystalloids in solution. 5. Nephrocalcinosis. The term refers to the deposition of calcium and phosphorus in the renal tubules or in the interstitial tissue of the kidney. The condition is characterized by hypercalcinuria, negative calcium balance and evidence in skiagram. It is often associated with the formation of calculi. 6. Prolonged immobility. When patients such as paraplegics are confined to bed for long periods unable to move their limbs, the bones tend to become decalcified and phosphate stones are often formed. DIABETIC NEPHROPATHY Diabetic Glomerulosclerosis The glomerular lesions of diabetic nephropathy are of three types: The nodules are usually situated at the periphery of the affected
glomerulus. These are eosinophilic and show a laminated appearance when
stained with periodic acid Schiff reagent. The initial lesion probably starts
within the capillary wall. The hya The diffuse glomerular lesion is more common than the nodular lesion and is the main cause of the reduced glomerular filtration rate and azotaemia characteristic of the later stages of diabetic glomerulosclerosis. The capillary walls are thickened by deposit of a substance rich in polysacharide. The basement membrane is probably first involved, with later extension to endothelial and epithelial cells. In the earlier stages, the changes are uneven within the same glomerulus and in different parts of the kidney. Later the whole glomerulus becomes hyalinised and bloodless and there is atrophy of the corresponding tubule. The diffuse lesion may occur without any evidence of nodular change but whenever there are nodular lesions, the diffuse change will be present in the other glomeruli. The exudative lesion is the least common and least characteristic
abnormality of the glomerulus in diabetic nephropathy. It consists of an
eosinophilic structureless crescentic area surrounding the periphery of a
lobule of a glomerulus. It stains more Other changes in diabetic nephropathy include usually severe renal vascular disease with hyaline change in the wall of arterioles and secondary areas of ischaemic atrophy. Pyelonephritis often occurs in diabetes mellitus especially in the later stages of diabetic nephropathy. Distal tubular or papillary necrosis is of frequent occurrence. ACUTE RENAL FAILURE Causes
Effects Uraemia is associated with headache, drowsiness, twitching of extremities, convulsions, coma and a group of other symptoms and signs. The features disclosed by biopsy are variable, but,there are renal lesions, degenerations of hypertrophic heart, cerebral edema, ulcerative ileocolitis and increased amount of urea in the renal cortex. Often bronchopneumonia is present as a terminal event. CHRONIC RENAL FAILURE Causes
Fanconi Syndrome Characteristics
The condition usually becomes apparent in early childhood and
death generally occurs before puberty. There is a widespread deposition of
cystine in different tissues (cystinosis), the cause of which is not known
although it implies a profound A similar entity generally referred to as adult Fancony syndrome has been found as a familial condition in adults. It is not associated with cystine deposition and presents as a form of osteomalacia. Such biochemical abnormalities as the aminoaciduria and glycosuria may be recognized prior to development of any clinical symptoms. NEPHROTIC SYNDROME The Nephrotic syndrome (or Lipid nephrosis) is a clinical complex consisting of :-
Etiology
Vast majority of the cases of nephrotic syndrome are idiopathic. Only rarely the cause is known. The following theories have been forwarded to explain the etiology of idiopathic nephrotic syndrome :- (i) A preceding streptococcal infection. In an established case of
nephrosis, subsequent recurrent streptococcal infections affect the disease
process adversely. Pathogenesis Once the glomerular lesion, i.e., abnormality of the epithelial foot processes and subsequent basement membrane thickening, is established, oedema in nephrotic syndrome follows proteinuria. Albumin is the main protein lost though other protein fractions like alpha and gamma globulins also are lost considerably. Proteinuria is mainly responsible for hypoproteinaemia. Protein intake is also low because of accompanying anorexia and diminished absorption of ingested proteins, because of intestinal oedema. This may further add to hypoproteinemia. Hypoproteinaemia leads to decreased colloidal osmotic pressure allowing escape of water into cellular tissue. This starts the oedema and sets up the factors which contribute further to accumulation of fluid in the body. The escape of water from plasma leads to reduction of blood volume leading to hormonal disturbances concerned with water and electrolyte regulation. There is increased secretion of antidiuretic hormone (ADH) and aldosterone. Aldosterone retains sodium and alongwith that more and more water is retained. However, the retained water cannot be held in circulation because of hypoproteinaemia and is lost to the extracellular tissue causing further reduction in blood volume and the whole cycle repeats. Like the interstitial tissue in all other organs, that of the kidney is also water-logged. This raises intrarenal hydrostatic pressure with its effect on venular patency. This raised internal venular resistance reduces the effective glomerular filtration and also increases tubular water absorption. The tense stretched capsule of the swollen kidney might be responsible for autonomic nerve stimulation causing afferent arteriolar spasm reducing glomerular filtration. The cause of hyperchlolesterolaemia is not fully understood. It is believed that it results from increased synthesis of cholesterol and of lipoproteins, and can be induced by certain nephrotoxic sera.
TUMOURS Classification
Renal Adenoma Gross Appearance Microscopic appearance. The tubules may be irregular or dilated, papillary processes may project into them. Some of the cells are small, dark or compact, but others may be large clear cells, so as to resemble those of the clear cell carcinoma. The capsule, if at all present may be penetrated by tumour cells.
Renal Carcinoma (Nephroma) Macroscopic appearance. The tumour arises in the upper or lower pole but more often in the middle portion of the kidney. It begins near capsule and enlarges to form a globular mass. Fibrous tissue may form a capsule around the tumour. The tumour is soft and in the cross-section is bulging, o yellow colour, bleeds freely and is often lobulated by fibrous trabeculae. There are numerous foci and masses of necrosis and haemorrhage; the tumour, often, compresses and distorts the pelvis and may invade it. Extension into the tributaries of the renal vein, into the main renal vein and even upto the vena cavae is not infrequent. Microscopic appearance. It varies greatly. The most common form is made up of large cuboidal or polyhedral cells with clear vesicular cytoplasm which may contain fat or glycogen. The nuclei are small, fairly dense and often eccentric. These cells grow in bands and papillary projections from a delicate fibrous reticulum. containing many capillaries which may give an alveolated character to the tumour. Necrosis, haemorrhage and blood pigment are common, other tumours are made up of smaller cells with granular cytoplasm and dense, centrally disposed nuclei. In these tumours, the cells are usually in sheets and masses. In either form acini may be found and these are often papilliferous, However, there may be mixtures of these types of cells with preponderance of one or the other. The supporting connective tissue is richly vascularized. Metastases are most frequent in lungs, liver, adrenals and bones and less frequent in kidney, spleen, heart and brain. Wilm's tuniours (nephroblastoma). This is the commonest malignant
tumour of early childhood. It usually occurs during the first three years of
life but may rarely occur in adults. It may attain an enormous size, nearly
filling the abdomen. Quite The tumour, which commences in the cortex, is 2 grey, soft and has a homogeneous character of a sarcoma. It tends to destroy the whole kidney and may spread to neighbouring organs. Distant metastases by the blood stream are not frequent. The microscopic appearance varies in different parts of the same tumour. The general character is sarcomatous. The cells may be round or fusiform. Glandular elements are often present; smooth muscle and striated muscle are not uncommon and in rare cases there may be cartilage and bone. CONGENITAL DISORDERS Classification
AGENESIS OF KIDNEY 1. Bilateral agenesis of kidneys is incompatible with life and is found only in still-born babies. 2. Unilateral agenesis is compatible with adequate renal function. The other kidney is enlarged in size. Causes 1. Unilateral absence of nephrogenic primordium. Pathology HYPOPLASIA Renal hypoplasia means the failure of the kidney to attain the normal
size. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||









|
Chapter 10 : Respiratory system ACUTE BRONCHITIS Etiology 1. The irritant may be bacterial, mechanical, or toxic. 2. Causative organisms:
3. May complicate any infectious fever, particularly typhoid. 4. Produced by dust, steam, poisonous gases and other irritants. Gross Appearance Microscopic Appearance CHRONIC BRONCHITIS Etiology 1. Chronic heart disease, valvular or myocardial, is probably the most important cause on account of continued congestion of the bronchial tree which weakens its resistance to bacterial infection from the nose and throat. 2. Infection in the nasal sinuses is another common cause. An antrum or a sinus may be a reservoir of infection from which the bronchi are continually being reinfected. The same is true of septic conditions in the oral cavity. 3. Dilatation of the bronchi, i.e., bronchiectasis is now k.iown to be a predisposing condition in many cases of chronic bronchitis. With dilatation of the lumen the condition becomes ideal for continuance of infection, for efficient drainage becomes difficult or impossible. 4. Cigarette smoking, when prolonged and persistent is related to chronic bronchitis. It interferes gravely with the beating of the respiratory cilia whose constant motion, when normal, keeps the bronchial tubes clean of mucus. Gross Appearance 1. Surface of the bronchial mucosa is dark red and appears
trabeculated. Microscopic Appearance BRONCHIAL ASTHMA Etiology Gross Appearance Microsopic Appearance 1. Mucosa thickened and oedematous. BRONCHIECTASIS Etiology 2. Obstruction Microscopic Appearance Complications
PNEUMONIA Classification based upon Etiology
Classification based upon Mode of Spread
Complications of Pneumonias
LOBAR PNEUMONIA Etiology Predisposing Factors
Pathology A. Stage of congestion 1. Lasts for about 2-4 hours B. Stage of red hepatisation
. C. Stage of Grey Hepatisation D. Stage of Resolution Complications
BRONCHOPNEUMONIA Etiology
Gross Appearance 1. Lobular consolidation patchily distributed; more often multilobar,
frequently bilateral and basal, at times involving single lobe. Microscopic Appearance 1.
Bronchi, bronchioles and adjacent alveolar space filled with
suppurative exudate containing neutrophils.
Fig 10.2 Bronchpneumonia Complications
LUNG ABSCESS Etiology
Gross Appearance 1. Diameter varies from a few.millimetres to 5-6 ceritimetres.
Microscopic Appearance 1. An acute abscess with dense infiltration of polymorphs and varying
number of mononuclear phagocytes. PULMONARY TUBERCULOSIS 1. Primary infection (Ghon lesion) 2. Secondary infection: Primary infection or Ghon lesion and etiology of tuberculosis have been described in chapter 6 on Granulomata. Healing with Fibrosis Chronic Fibrocaseous Tuberculosis 1. Cascous tissue breaks down and a cavity forms. The characteristics of fibrocaseous tuberculosis, thus are: 1. Consolidation and caseation Microscopic Appearance Acute Tuberculous Caseous Pneumonia 1. Lesions ulcerate through the bronchial wall in many places and the
infection spreads widely throughout the lung by inhalation. Microscopic Appearance Acute Miliary Tuberculosis 1. Results when a caseous focus discharges its contents into a blood
vessel. Microscopic Appearance 1. Tubercles seen all over the lung framework. PULMONARY INFARCTION Etiology There are two varieties, the embolic and thrombotic. The embolus may consist of :- Pulmonary thrombosis may occur in: Predisposing Causes 1. Cardiac diseases - mitral steriosis, bacterial endocarditis
Gross Appearance Microscopic Appearance ATELECTASIS Types 1. Atelectasis neonatorum Primary (Congenital) Atelectasis Etiology Gross Appearance Microscopic Appearance Secondary Neonatal Atelectasis Etiology Gross Appearance Microscopic Appearance Acquired Atelectasis Etiology
Gross Appearance 1. May involve all lobes (acute massive collapse leading to death after
abdominal operations) but most often is lobar or segmental. Microscopic Appearance 1. The collapsed alveoli become slit-like; lung appears to have too much
tissue and too little air. EMPHYSEMA Pathogenesis Increased intra-alveolar pressure is the more important factor. This pressure is increased due to trapped air. It is generally believed that trapping of air is as a result of obstruction of the small bronchi and bronchioles by plugs of mucus. The obstruction is of the check-valve type, which allows air to be drawn in during inspiration but prevents it from passing out during expiration. Obstruction may be spasmodic or permanent. Spasmodic obstruction is exemplified by paroxysmal bronchial asthma, in which the development of emphysema is a constant threat. The majority of cases of emphysema, however are slow and insidious in onset. It is hard to visualize a 4. plug of mucus, remaining unaltered in a - small bronchu s and acting as a check valve over long periods. It is possible that the basic lesion is an obliteration of the bronchioles from bronchiolitis and that the air enters and leaves the alveoli by the back door route of pores of Cohn, by which entry of air from neighbouring lobules, occurs more readily than does exit. If such a person has a chronic cough, there is distension of alveoli with destruction of their walls. The mucus plugging of bronchial passage is prevented normally by the ciliary movements. The health of the cilia may be interfered with by viral infections, e.g., influenza, by bacterial infections tuberculosis and chemical agents, e.g., toxic gases. Impaired nutrition of the alveolar walls will impair their elasticity. This impairment may be a result of ischaemia. This weakness of alveolar wall is another factor in the pathogenesis of emphysema. Types of Emphysema
Chronic Obstructive Emphysema Types 1. Centrilobular emphysema. The central or proximal parts of acini
are affected, while distant alveoli are spread. This is the commonest
type. Microscopic Appearance
Compensatory Emphysema The term compensatory emphysema is misnomer as there is no necrosis, an essential feature of emphysema; the better term is compensatory overinflation. Senile Atrophic Emphysema Interstitial Emphysema BRONCHOGENIC CARCINOMA Gross Appearance They may represent, in part, different stages of the same process. B. Diffuse infiltrating form The turnour masses are found irregularly distributed throughout the lung, poorly vascularised, pallid and necrotic, of irregular size sometimes fusing to form large masses. C. Peripheral form . 1. Less frequent; arising from a small bronchus. D. Miliary carcinosis There are innumerable nodules, a few millimeters in diameter, usually situated along the course of lymphatic vessels. Associated findings (common to allforms) Microscopic Appearance There are three histological types. B. Anaplastic (Small cell or reserve cell carcinoma C. Adenocarcinomatous (Adenocarcinoma). A. Epidermoid carcinoma: 1. Shows marked differentiation.
. Such areas are frequently seen in the bronchial lining quite apart from
the presence of bronchiectasis. B. Anaplastic carcinoma: C. Adenocarcinoma:
Spread ALVEOLAR CELL CARCINOMA 1. Often
diffuse; may affect both the lungs; yet localised excisable tumours may
occur.
Fig. 10.6. Alveolar Cell Carcinoma
BRONCHOADENOMA
Fig 10.7 Bronchoadenoma 1. Characterised by its long duration with repeated
haemorrhages. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||






|
Chapter 11 : Alimentary system PEPTIC ULCER Etiology 2. Trauma. Rarely onset of symptoms occurs shortly after blow to upper abdomen. 3. Infarction or vascular theory. Based upon: Gross Appearance A. Acute Peptic Ulcer B. Chronic Peptic Ulcer Microscopic Appearance Complications
TUMOURS OF STOMACH Classification
CARCINOMA OF STOMACH Etiology Gross Appearance A. Large cauliflower (Fundal polypoid) type :
2. Ulceration of surface gives rise to infection and haemorrhage. B. Malignant Ucer (Antral excavating) type: 1. Tumour is only slightly elevated and becomes ulcerated
early. C. Diffuse infiltrating (Leather bottle) type: 1. No real tumour is seen but there is great thickening of the
stomach wall. Microscopic Appearance B. Anaplastic type: Spread
REGIONAL ILEITIS Etiology The predisposing factor is emotional stress. Gross Appearance Microscopic Appearance ULCERATIVE COLITIS Etiology Etiology unknown: Gross Appearance 1. Rectum and sigmoid colon most commonly affected; en6re colon may be affected; at times disease is restricted to right side of colon (segmental colitis) or occasionally the terminal ileum (reflux ileitis). 2. Ulceration, begins in the rectum at tips of the mucosal folds immediately over the longitudinal muscle bands. 3. The mucosa is intensely congested and bleeds easily. 4. Later the ulcers coalesce, giving rise to larger irregular areas of denudation of mucosa, the floor of which is formed by circular muscle fibres. 5. Between the ulcers especially in long standing cases, islands of swollen hyperplastic mucosa persist. 6. In some cases numerous polypoid masses are seen (pseudopolyposis). 7. There may be extensive mucopurulent discharge and haemorrhage from the ulcerated areas. 8. Attempts at healing take place during remissions but fibrous thickening and stenosis of lumen are uncommon. 9. During relapses, the colon is markedly spastic and normal sacculation is lost at an early stage. Microscopic Appearance 1. The earliest lesions found in the mucosal crypts, which become
distended with polymorphs, cosinophils, red cells and mucus. These lesions
are called crypt abscesses. AMOEBIC COLITIS Etiology Gross Appearance 1. The organisms enter the wall of colon through the mucosa ad settle in the submucosa where they liberate oroteolytic enzyme causing tissue necrosis. 2. The first visible lesion is the formation of swollen, congested patches in the mucosa, central parts of which become soft and yellowish, as necrosis occurs. 3. The mucosa then gives way and an ulcer is formed with undermined margins. 4. Such ulcers, as they spread, become confluent first in their deeper parts. 5. The bridges then give way and ulcerated areas are greatly increased. 6. A considerable part of the bowel may thus have lost its mucosa while in the intervening parts, fragments of mucosa in process of disintegration and separation are present. 7. Gangrene of the mucosal patches may be superadded. Microscopic Appearance Complications
Ulcerative Colitis vs. Crohn's
Disease 1. Affects mainly the Peyer's patches and solitary follicles in the
lower part of ileum. Microscopic Appearance 1. Enlargement of Peyer's patches due to congestion and a great increase
of nongranular cells derived from reticuloendothelial cells which have become
swollen and spherical. VIRAL HEPATITIS Types Infective Hepatitis Gross Appearance Microscopic Appearance 1. Widespread necrosis of parenchymal cells. 3. Inflammatory cells and often polymorphs are seen in the portal areas;
there may be endophlebitis of portal veins. Serum Hepatitis Yellow Fever Microscopic Appearance LIVER CIRRHOSIS Types Portal cirrhosis 5. Infections Gross Appearance 1. Liver initially much larger due to fatty change; later
atrophic. Microscopic Appearance Post-necrotic Cirrhosis Etiology Gross Appearance 1. Liver firm, with nodular surface. Microscopic Appearance Biliary Cirrhosis B, Primary biliary cirrhosis Gross Appearance 1. Liver enlarged and green. Microscopic Appearance Stage I : Florid duct lesion Stage II : Ductular proliferation Stage III : Scarring Stage IV : Cirrhosis Complications of Liver Cirrhosis GALL STONES Types of Gall Stones Characteristics Pigment Stones Mixed Stones (i) Composed of. (a) Cholesterol (b) Bile pigment (c) Calcium (d) Proteins. (ii) Always multiple Formation of Gall Stones Three factors play a role in the formation of gall stones. 2. Stasis. Stasis facilitates the lying down of various constituents of the stones while continuous stream prevents it. In pregnancy, the gall bladder does not empty in response to a fatty meal. Thus gall stones are commoner in the women, especially in multipara. Stasis may also lead to infection which further predisposes to the stone formation. 3. High bile cholesterol. Deposits of cholesterol in the mucosa may become pedunculated detached and form the starting point of calculi. Complications I. Local: B. Stone passing outside the gall bladder II. General: ACUTE CHOLECYSTITIS Etiology 1. Causative organisms: 2. Chemical irritants: (i) Bile salts (ii) Acids. 3. Cystic duct occlusion: Gross Appearance Microscopic Appearance CHRONIC CHOLECYSTITIS Etiology Gross Appearance 1. Bluish colour of normal gall bladder is lost, surface may be
opaque. 5. Obstruction may result from inflammatory oedema, cicatericial
contraction or impaction of stone at the neck leading to dilatation and
thickening. 7. The bile pigment is absorbed and no more can enter owing to
obstruction. Microscopic Picture 1. Marked lymphocytic infiltration with some plasma cells and
eosinophils. CHOLESTEROLOSIS OF GALL BLADDER Etiology 1. Abnormal absorption of cholesterol from the bile by epithelial
cells of gall bladder. Gross Appearance 1. Wall usually a little thickened. Microscopic Appearance
3. When the deposit becomes more massive, these cells may die; release of lipids gives rise to the precipitation of cholesterol crystals in the subepithelial region and a subsequent inflammatory reaction of white cells, giant cells and fibroblasts. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
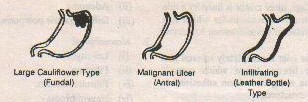

|
Chapter 12 : Miscellaneous topics BREAST DISORDERS Selerosing Adenosis (Fibrosing Adenosis) Etiology 1. Commonly follows
incomplete involution after an interrupted pregnancy or lactational. failure.
Gross Appearance 1. In early stages,
grey firm nodules a few Microscopic Appearance The nodule is well defined
but not. encapsulated. 1. Florid phase. There is
oedema and irregular proliferation of both epithelial and myoepithelial
elements. 4. Phase of fibrosis. Fibrosis ultimately dominates the picture leading to atrophy. The acini have a tendency to break up into small groups or clumps of cells. At this stage, it is easily mistaken for carcinoma in frozen sections.
, Collagen Tissue Classification of Breast Tumours I. Benign tumours
2. Duct papilloma. II. Malignant tumours
Benign Tumours Sarcoma(i) Primary (ii) Generalised. Fibroadenoma. A fibroadenoma occurs chiefly in young women originating perhaps at puberty and growing during the years of developing sexual activity. It is commoner in nulliparae than in those who have borne children. It is slowly growing tumour but growth may be more rapid during adolescence, in pregnancy and towards menopause. Two varieties are recognised. - The intra-canalkular fibroadenoma is the commoner variety. As the hyperplasia involves particularly the specialised. connective tissue of the lobules, the tumour is more of a fibroma than an adenoma. It is usually well encapsulated, has a soft consistence and a rather moist appearance. The cut surface may show many narrow slits, sometimes little masses can be distinguished enclosed within small spaces. The encapsulation may be only partial the tumour blending on one side with the surrounding breast tissue. Microscopically, there is a great proliferation of loose connective tissue of open structure which invaginates the wall of the duct projecting into the lumen to form polypoid masses, and producing great dilatation, elongation and distortion of the ducts. The ordinary connective tissue stroma of the breast takes no part in the overgrowth. The lobules of the surrounding tissue often show hyperplasia. The pericqnalicular fibroadenoma is a much harder tumour and seldom becomes as large as the preceding variety. it is well encapsulated and has a characteristic mobility when palpated. The cut-surface is white, dry and homogeneous. Microscopically there is a proliferation of glandular and fibrous tissue. The new connective tissue surrounds the ducts without invaginating them. The picture suggests less active growth than that of the preceding variety. The distinction between the two forms, however, is not fundamental. No fibroadenoma is entirely of one variety. The division is made on the basis of predominant lesion, Duct-papilloma
(Adenocystoma). The papilloma projects into a Mated duct, usually in the
nipple. At first it is composed of a series of folds but as it increases in
size the folds or villi adhere together so that the surface becomes
relatively smooth. Finally, it descends the ducts and becomes a solid compact
mass. Carcinoma of Breast Carcinoma of breast is of
five types; Scirrhous Carcinoma. This is the commonest form of mammary growth occurring in women between the ages of thirty five and sixty five. The growth is situated most often in the upper outer quadrant of the breast. Usually, the growth arises in the substance of the gland fairly close to the nipple, but occasionally an outlying lobule is affected first. Both breasts may be affected simultaneously or in succession. The tumour is mall in size but invading the breast in all directions and it has no capsule. It is fibrous and light grey or pinkish grey in colour. Scattered through the tumour, there are often pale fibrous streaks and pinhead yellow spots of necrotic epithelial tissue. Microscopically, the tumour is composed of spheroidal epithelial cefis in a stroma of fibrous tissue. The spheroidal cells are believed to be derived firom ductal epithelium. The stroma is abundant and composed of tough fibrous tissue. The elastic lamina of the ducts shows striking overgrowth. Stroma is less dense, often, towards the periphery of the tumour and the epithelial cells are present in great number.
Atrophic scirrhous
carcinoma but very
hard and fibrous and fixed to adjacent structures. Metastasis is very
late. Microscopically there are small islands and delicate strands of
spheroidal epithelial cells, embedded in dense fibrous tissue. Adenocarcinoma. This is a rare tumour of the breast. In its fully differentiated form, it is of soft consistence and may become quite bulky; but is of slow growth, low malignancy and may remain localised for a long time. The microscopic appearance is that of gland spaces surrounded by columnar epithelium. Duct-carcinoma. This tumour usuaUy arises from one of the large ducts near the nipple. The growth may originate from duct papilloma. Owing to fusion of the papiflary processes, a gland like condition way be produced. The tumour is only slowly invasive. Bleeding from nipple is a common complaint. Paget's disease. The disease begins with a
chronic eczema of the nipple. After some years, cancer ofThe atrophic
scirrhous carcinoma is an extremebreast develops. The skin lesion is
malignant, but variety of the ordinary form. It is found in shrivel- I of
very slow growth and without glandular involveled breasts, especially in old
age and forms a tumour ment. The breast tumour may be rapid growth. The
Microscopically, the skin in the affected area shows marked epidermal hypertophy before ulcerationtakes place. The most characteristic feature is the presence of peculiar structures known as Paget'scells. There are large, clear, vacuolated cells withsmall pyknotic nuclei. They look like clear spacespunched out of the epidermis. They are most abundant in the basal layers, but may permeate theentire thickness of the epidermis. The underlying dermis shows infiltration with lymphocytes andplasma cells. In the later stages, there is ulceration of the epidermis. BONE TUMOURS Osteogenic tumour: (ii) Osteosarcoma (osteogenic sarcoma) Chondrogenic tumours:
Collagenic tumours:
Myelogenic tumours.
Osteogenic Sarcoma Etiology 1. Occurs commonly
in second decade of life. Gross Appearance 1. Fusiform mass at the
end of the bone which fades away on the shaft. Microscopic Appearance 1. Tumour cells are
osteoblasts of three types: (ii) Large spindle cell. (iii) Polyhedral cell. 2. Giant cells of tumour or foreign body type. Giant Cell Tumours (Osteoclastoma) Etiology 1. Occurs commonly between 20-30 years of age. 2. Important predisposing factor is trauma. 3. Usual sites ate lower end of femur, lower end of radius, upper end of tibia; occasionally bones of jaw and skull. Gross appearance 1. Soft, dark red,
haemorrhagic mass, sometimes with yellowish areas. Microscopic appearance 1. Spindle shaped cells, incorrectly termed as stromal cells, but are really the basic mononuclear cells of the tumour.
2. Multinucleated giant cells of osteoclast type which are largest of all giant cells. 3. The giant cells may represent a development of the mononuclear spindle cells, perhaps representing an absorption phase of activity. The tumour tends to become
malignant. Ewing's Tumour Etiology
2. Males more commonly affected. 3. Affects diaphysis of bones usually upper and lower parts of femur and tibia, upper parts of humerus and fibula, and pelvis. Gross Appearance 1. Very soft,
resembling brain tissue. Microscopic Picture 1. The cells are round or polyhedral. 2. Very uniform in
appearance with round nucleus and ill-defined cytoplasm.
|
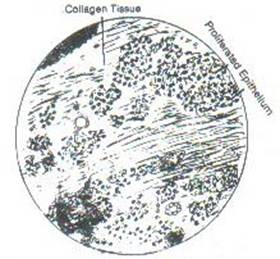
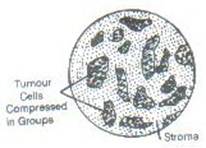


|
Chapter 13 : General Bacteriology
MORPHOLOGY OF BACTERIA Microscopy 2. Technique: (i) Cover the hollow
with a thin layer of vaseline
Brand Petroleum Jelly. B. Dark-ground illumination
2. The microscope has a
special condenser in which lenses are arranged so that direct rays of light
are stopped and the material under view is illuminated by oblique rays. C. Electron microscopy 1. Magnifications
upto 200,000 can be obtained. 3. The suspension of material is dried on a very thin cellulose film through which the beam passes and the image can be seen. Shape of Bacteria 1. Coccus. A spherical form; at times oval; may be arranged in long. chains, pairs or clusters, depending upon the mode of division. 2. Bacillus: (i) A cylinderical
rod. 3. Vibrio. Cylinderical form slightly bent or curved on itself frequently resembling a comma (,). 4. Spirillum. Much like vibrio but with multiple bends or spirals. 5. Actinomyces. With
long branching filaments or mycelia. Size of Bacteria 1. Measured by a
special micrometer eye piece. Bacterial Capsule 1. Bacteria may have readily demonstrable capsules, e.g., Pneumococcus, Friedlander's Flagella bacillus, a loose undemarcated secretion termed slime layer or too thin a capsule to be seen under optical microscope when it is termed microcapsule. Demonstration of Capsule
3. Functions of Capsule:
Bacterial Spore 1. Oval or spherical
bodies within the protoplasm, difficult to stain; also termed endospores.
Flagella 1. Thin, delicate, long threads which appear to pierce the cell wall; help in motility. 2. Position of flagella
(ii) Prolonged incubation
4. Flagella are complete antigens and consist of protein. Reproduction 1. Multiply by division or simple fission; no true sexual phase. 2. Line of cleavage is at right
angle to long axis in cylindrical forms. Cocci tend to become elliptical
immediately before division. In many cases the young forms are coherent till they reach adult
size. CULTIVATION OF BACTERIA Fluid Media (Broth) 1. Meat extract
broth 2. Digest broth 3. Peptone water
Solid Media 1. Gelatin media. Gelatin melts at high temperatures. Thus gelatin media are too difficult to handle and sterilize. 2. Agar (Agar-Agar) media:
Enriched Media Simple media (broth or agar) are at times unsuitable for growth of parasitic bacteria, e.g., pneumococcus, gonococcus, influenza bacillus. The same may be enriched by addition of :- 1. Serum 10% 2. Blood 5-10% 3. Ascitic fluid (10%) 4. Glucose (1-2%). The melted agar should be cooled to a temperature of 50-55°C before enriching. Above this temperature proteins become coagulated; below this temperature, there may be premature setting. Selective Media 1. Chocolate Agar (ii) by liberating the contents of corpuscles. 2. Dorset's egg medium 4. Special selective
media. Anaerobiasis 1. Deep agar tubes Bacteria intended to be grown are inocculated in deeper part of solid media. 5% glucose is added as a reducing agent. 2.
Brewer's medium
3.
Glucose broth 4. Robenson's cooked meat
medium 5. Reduced iron medium
6. Mc Intosh and Filde's
jar DESTRUCTION/ELIMINATION OF BACTERIA Methods
Employed 1. Light 3. Electricity
B. Chemical agents:
Bacterial filters: 2. Chamberland
filters IMMUNITY Types of Immunity B. Acquired:
(i) Natural (ii)
(ii) Artificial.
Natural Immunity
(a) Skin. Skin is impervious to bacteria. (ii) Others require definite breaches in skin continuity, e.g., streptococci, Clostridium tetani. (iii) Extensive traumatic lesions are necessary for Clostridium welchii (gas gangrene organism).
(b) Mucous membranes
(c) Secretions (i) Gastric juice
being acidic is bactericidal. Species Immunity 3. Some diseases of animals do not occur in man,
e.g., rinderpest, Johne's disease of warm 4. Cold-blooded animals are generally not susceptible to
disease of warm-blooded animals. Racial Immunity 1. People of tropical regions are more resistant to yellow fever than others. 2. Coloured races are more susceptible to tuber culosis
than white people. malaria. Individual Immunity 1. People with sound
health are more resistant to infections than debilitated people. Active Immunity A. Natural 1. Single attack of an
infectious disease may confer life-long immunity, e.g., smallpox, chickenpox.
B. Artificial active immunisation 1. By living attenuated
organism, e.g., anthrax vaccipation, smallpox vaccination, rabies
vaccination, B.C.G., yellow fever vaccination, oral poliomyelitis
vaccination. Passive Immunity A. Natural 1. Transplacental
passage of immune bodis from the mother to the foetus. B. Artificial passive immunization by immune serum 1. Antitoxin sera. Diphtheria, tetanus 2. Antibacterial sera. Pneumococcal pneumonia, meningococcal meningitis 3. Antiviral sera. Measles, poliomyelitis, yellow fever
ANTIGENS AND ANTIBODIES Antigens An antigen may be defined as a substance which when introduced into animal tissue, stimulates the production of substances (known as antibodies) which react specifically with the original substance introduced. The common substances which may act as antigensare bacteria, blood corpuscles, serum, bacterial toxins, vegetable toxins. Haptenes are the partial antigens which fail to stimulate the production of antibodies but can react in vitro with the serum prepared against their organism. Barring haptenes of pneumococci which are complex carbohydrates, all the antigens are generally proteins. For being an antigen, the protein must be: 1. Foreign to the animal
injected Antibodies
(Immunoglobulins) 3. Bacteriolysin. An antibody causing lysis and disintegration of bacteria. 4. Bacteriocidin. An antibody that kills the bacteria without producing lysis. 5. Antitoxin. An antibody that neutralizes the toxic effect of a toxin. Chemically the antibodies are globulins, mostly gamma-globulins. Site of Production The antibodies are thought
to be produced by the following
types of cells. (iv) In the bone marrow Classes of Immunoglobulins
Human sera contain IgG, IgA, IgM, IgD and IgM in descending order of concentrations. Auto-antibodies Under some circumstances the body develops antibodies capable of reacting with antigens of the same individual. Such antibodies are termed autoantibodies and presumably result from post-natal somatic mutation of the antibody producing cells. These antibodies are associated with a group of disorders called auto-inintune diseases which include haemolytic anaemia, thrombocytopenic purpura, chronic thyroiditis, Addison's disease chronic pancreatic disease and heart disease. ANTIGEN-ANTIBODY REACTIONS 1. Agglutination or clumping 2. Precipitation or flocculation 3. Lysis or disintegration 4. Destruction 5. Complement fixation 6. Phagocytosis or intracellular digestion 7. Neutralization. Agglutination The antigen inducing agglutination is termed agglutinogen, the corresponding antibody aggititinin and the resultant clumps agglutinate. The medium in which agglutinogen and agglutinin react is termed menstrum. The incomplete or monovalent antibodies do not cause agglutination, though they may combine with the antigen and block it preventing agglutination if suitable agglutinin is added later. Techniques ofAgglutination 1. Slide test. A thick suspension of antigen and the antiserum are mixed thoroughly on a glass slide and observed through naked eye, hand lens, or low power of the microscope. Slide test is none too conclusive and is used as a mass screening test. 2. Tube test. The bacterial suspension, standardised to the required opacity is tested against serial dilutions of serum. The highest dilution of the serum in which agglutination is visible is called the titre of the serum. Applications ofAgglutination Reaction 1. Widal test for typhoid 2. Weil-Felix reaction for typhus fever 3. Paul-Bunnell test for infectious mononucleosis 4. Cold-agglutination test for primary atypical pneumonia 5. Coomb's test for Rh antibodies 6. Haernagglutination test for blood group typing 7. Urinary human chronic gonadotrophin test for pregnancy., Precipitation The antigen participating in precipitation reaction is known as precipitinogen and the antibody precipitin. Differences from Agglutination 1. In agglutination, antigen is a suspension of relatively large particles; in precipitation it is an extremely fine colloidal solution. 2. In agglutination, the agglutinate is formed largely from the antigenic suspension; in precipitation, precipitate is formed mainly by the serum globulin, i.e., the antibody. 3. Precipitate is at times soluble; it may readily dissolve by changing the physical conditions of the test, e.g., a temperature over 55°C. 4. In agglutination test a ~tandard concentration of antigen is tested against serial dilutions of antibody; in precipitation a standard concentration of antibody is tested against serial dilutions of the antigen. Applications of Precipitation Reaction 1. Precipitation reaction
is more sensitive and specific reaction for detection of antigen and is
applied in medico-legal laboratories for: 2. C-reactive
protein test Lysis (Disintegration) and Destruction 1.
Bacteriolysis
(ii) Involution forms followed by disintegration also result when normal guinea pig is inoculated intraperitoneally with vibrios premixed with immune serum even if the serum has been heated at 70°C for one hour (Pfeiffer's phenomenon). The reaction of bacteriolysis is limited to some Gram-negative bacilli. 2. Haemolysis (Cytolysis)
Bacterial Destruction Similar to bacteriolysis, but in this type of reaction bacteria are killed without undergoing disintegration. Complement Fixation Apart from antigen and antibody, another factor is also involved in antigen-antibody reaction. This factor is known as Complement and consists of at least four components; C, and C2 are heat labile whereas C3 and C4 are heat stable. Complement is found in the normal serum of all animals; guinea pigs have most marked and constant quantities of complement and serve as a source for laboratory purposes. Complement Fixation Test If complement is added to antigen-antibody mixture it completes the antigen-antibody reaction and getsfixed in the process. A further addition of red blood corpuscles (usually sheep RBQ and haemolysin does not result in haemolysis as complement is no longer available in fixed form. If however, the antigen and antibody in the original mixture are not specific for each other, they fail to fix the complement and lysis of RBC results. This is known as complement fixation test. Complement fixation test can be applied in two ways :- 1. With a known antigen and an unknown serum, e.g., Wassermann reaction for syphilis. 2. With an unknown antigen and known serum. Phagocytosis The cells involved in phagocytosis of bacteria are of two types: 1. Microphages, which are mainly polymorphs. 2. Macrophages comprising the large mononuclears and endothelial cells. However these cells are unable to ingest (phagocytose) the bacteria in the absence of serum indicating that one or more substances in the serum contribute to the process of phagocytosis. Two such substance are: 1. Opsonins, inactivated by heating at 55°C 2. Bacteriotrophins, heat stable. Toxin-Antitoxin Neutralization Toxin are antigenic and when introduced into the body stimulate the production of antitoxins. An antitoxin neutralises the effect of toxin on the body. Applications of Neutralization Tests 1. Shick test for diphtheria. 2. Anti-streptolysin-0 test for streptococcal infections. HYPERSENSITIVITY Hypersensitivity means a
susceptibility of an organism to substances which give rise to little or no
reaction in normal members of
the same species. It is
divided in three groups: 2. Atopic hypersensitivity, e.g., asthma, hay fever, urticaria. 3. Bacterial allergy (delayed hypersensitivity), e.g., tuberculin reaction, Frei-test (in lymphogranuloma venereum) and Casoni test (in hydatid disease). |
|
Chapter 14 : Systematic bacteriology STAPHYLOCOCCUS Species 2. Staph. albus 3. Staph. citreus Habitat Morphology 2. Size. 0.7-1.2 µ 3. Arrangement 4. Motility. Non-motile
Cultural Characteristics 1. Grow readily on the usual media; temperature range 12-44°C, optimum temperature 37°C 2. Facultative
anaerobes, i.e., multiply both in aerobic and anaerobic conditions. 6. On blood agar plate. Pathogenic strains usually but not always show partial or complete haemolysis in the atmosphere with high carbon dioxide content. Occasionally haemolysis may be observed with non-pathogenic strains. Biochemical Activity 1. Ferment lactose, glucose, maltose, glucose and mannitol with acid production but with no gas. Mannitol is generally fermented by Staphylococcus aureus - a property that distinguishes it from non-pathogenic strains. 2. Proteolytic activity. Staphylococcus aureus liquefies gelatin more frequently than nonpathogenic cocci. Indole is not produced. 3. Catalase positive. Toxin Production 1. Alpha toxin (i) Most important of all
toxins and produced in high carbon-dioxide environment. 2. Beta toxin: 3. Delta-toxin: 4. Leucocidin. Destroys
white blood cells. Pathogenicity (vii) Wound and burn sepsis. Deep infection: (vi) Perirenal abscess. 3. Gastrointestinal
infections: Coagulase Test 1. Tube method. Human plasma is diluted 2-4 times with saline and inoculated heavily with the organism. A known positive organism is similarly tested as a control. The tubes are incubated at 37°C. If coagulation occurs in 2-5 hours, the organism is coagulase-positive. 2. Slide method: The organism is mixed with a drop of plasma on the glass slide. If plasma coagulates the organisms is coagulate positive. Coagulase-positive (or coagulase producing) organisms usually from aureus pigment, and are termed Staphylococcus aureus. Such organisms are pathogenic. Coagulase negative organisms are nonpathogenic and include Staphylococcus albus and Staphylococcus citreus.
Organisms are grown on an agar medium containing phenolphthalein diphosphate in a petridish. If the organisms produce phosphatase, phenolphthalein is liberated free and can be detected by pink coloration on exposure to ammonia vapours. STREPTOCOCCUS Species 2. Strept. viridians 3. Strept. faecalis Morphology 4. Motility. Nomnotile
Cultural Characteristics 1. Pathogenic species do not grow well on ordinary media and require enrichment with serum, ascitic fluid or blood; nonpathogenic species, e.g., Streptococcus faecalis grow luxuriously on ordinary media. 2. Optimum
temperature 37°C, range 20-42°C 3. Facultative anaerobes; grow best in the presence of free oxygen; some strains are microaerophilic (often called anaerobic though erroneously). 4. In fluid media.
(ii) Non-haemolytic
strains give well marked general turbidity with only a slight deposit.
Strains with long chain tend to give a deposit, those with short chains, general turbidity. 5. On solid media: (b) On blood agar.
Three types of appearances: On repeated subcultures on blood agar the virulence of the organism may be lost without alteration in the appearance of colonies (Matt attenuated); at times, such loss of virulence may leave the colonies smooth, regular and glossy. This change in appearance is associated with "M" type specific antigen. Biochemical Activity 1. Ferment carbohydrates with acid production 2. Pigment not formed 3. Indole not produced 4. Gelatin usually not liquefied except by some faecalis strains - 5. Some faecalis strains produce H2S 6. Litmus milk acidified; clotted by faecalis strains. Serology Antigenic structure of streptococcus is extremely complex and has three well-defined components: 1. Type-specific
protein "M" which is stable and related to virulence. On the basis of precipitation reaction with group specific "C" antigen present in the cell wall, haemolytic streptococci are divided in 18 Lancefield groups (Groups A. B, C, D, E, F, G, H, & L, M, N, 0, P, Q, R, S, T). All the human strains are found in Group A which on further typing with type specific "M" Protein is divided into 55 types (types 1, 2, 3, etc.) Classification The streptococci are classified into α, β, γ-streptococci on the basis of appearance in blood agar. α -(viridans group) and γ-(enterococcus group) are further classified into species on the basis of physiological and biochemical activities. β-haemolytic streptococci are classified as described under serology. Toxin Production Toxin produced are:
These toxins are produced by haemolytic streptococci, particularly of group A. Dick test Pathogenicity A. Streptococcus haemolyticus
12. Secondaary infections, e.g., bronchopneumonia following measles, whooping cough and influenza. B. Streptococcus viridans
2. May cause sepsis following tooth extraction and subsequent bacteraemia; on previously damaged heart valves, bacteraemia causes subacute bacterial endocarditis. C. Streptococcus faecalis
Schultz-Charlton Reaction Intradermal inoculation of
serum, collected from convalescent cases of scarlet fever, into a patient
showing the erythematous rash results in local blanching. Immunization Against Scarlet Fever A. Active immunization
B. Passive immunization
PNEUMOCOCCUS Species Morphology
(ii) Capsule demonstrable as a clear hole in Indian ink preparation.
Cultural Characteristics 1. Grow only on enriched media; temperature range 25-42°C; optimum temperature 37 °C. 2. Aerobes and facultative anaerobes; growth improved by 5-10% CO2. 3. Optimum pH 7.8, range 6.5-8.3. 4. In blood agar. 5. In fluid media, e.g., glucose broth, there is form turbidity. Rapid autolysis due to activity of intracellular enzymes. Autolysis enhanced by bile salts and sodium lauryl sulphate Biochemical Activity 1. Ferments lactose, maltose, glucose, sucrose and inulin with acid production. 2. Gelatin not liquefied. 3. Indole not formed. Serology Pneumococcus contains two main antigenic components. 1. A nucleoprotein, common to all types. 2. A type specific polysaccharide termed specific soluble substance (S.S.S.) because it diffuses into the culture medium or infective exudates and tissues. Pneumococci isolated from cases of lobar pneumonia are divided into 4 types, I, II, III and IV. On further serotyping, about 80 serotypes are known. Pneumococci can be typed
by: 2. Precipitation of the specific soluble substance with the specific serum. 3. Capsule-swelling reaction.
Toxin Production 1. Pneumococcus does not produce a soluble toxin; the toxic symptoms in pneumococcal infections are associated with specific soluble substances present in the capsule; noncapsulated forms are avirulent.
2. Haemolysin (oxygen liable) and leucocidin are produced but these are too weak to contribute to virulence. Pathogenecity Pneumococcus is commensal in the mouth and nasopharynx of many healthy persons. It produces: 1. Lobar pneumonia 2. Bronchopneumonia 3. Empyema 4. Otitis media 5. Meningitis 6. Arthritis 7. Endocarditis 8. Sinusitis 9. Primary peritonitis in children. Bile Solubility Test Addition of bile (or bile salt) to the broth culture of pneumococcus results in lysis of the organisms. 2-4 drops of sodium desoxycholate (1:100) are added to 5 ml of a broth culture of suspected pneumococcus (pH6.6) The mixture is allowed to stand at 37°C The pneumococcal culture gets cleared in 10-15 minutes. Optochin Sensitivity Test Quelling Phenomenon This is employed for
typing of pneumococci prior to serum therapy in lobar pneumonia. Sputum is mixed with a drop of each serum on a glass-side
and covered with a cover-slip. After about 5 minutes, the slide is examined
under a microscope. NEISSERIA Species 1. N. gonorrhoeae 2. N. meningitidis. Morphology 1. Shape. Spherical or oval cocci. 2. Size. 0.6 x 0.8µ 3. Arrangement. In pairs with adjacent sides flattened. Long axis of the coccus is at right angle to axis joining the two cocci. 4. Motility. Non-motile. 5. Spores. Non-sporing. 6. Capsules. Non-capsulated. 7. Staining. Readily stained by aniline dyes; Gram-negative. Cultural Characteristics 1. Do not grow on ordinary media. 2. Grow on media enriched with animal protein such as blood, serum or ascitic fluid. 3. Strict aerobes; growth improves in presence of 10% CO2 and high humidity. 4. Optimum pH 7.4-7.6. 5. Optimum temperature 37°C. 6. In fluid media, growth is poor with a slight granular deposit with little general turbidity. 7. On solid media. The colonies are: (i) Small (0.6-1.0
mm in N. gonorrhoeae, 1-2 mm in N. meningitidis) with regular edge. Biochemical Activity Very little biochemical activity 1. Ferment some carbohydrates with acid production. Maltose is fermented by N. meningitides but not by N. gonorrhoeae 2. Gelatin not liquefied. 3. Indole not produced. 4. No change in litmus milk. Neisseria gonorrhoeae (Gonococcus) Serology Gonococcus has a complex antigenic structure with a group polysaccharide and a group nucleoproteins. Two types, type I and type II are described with numerous subtypes. Type I includes most of the strains from acute cases.
Pathogenicity Causes gonorrhoea in human beings only.
Nelsseria Meningitidis (Meningococcus) Serology Meningococcus has a complex antigenic structure with :- 1. Group specific polysaccharide 2. Group specific nucleoprotein 3. Type specific polysaccharide Toxin Production Meningococcus produces an endotoxin which is difficult to demonstrate. Pathogenicity 1. Cerebrospinal meningitis. 2. Chronic meningococcal septicaemia ESCHERICHIA Species Escherichia Coli
Habitat Widely distributed in nature; present in faeces of man and animals, soil, and surface water.
Morphology 1. Shape. Rods with rounded ends. 2. Size. 1.3 x 0.6µ 3. Arrangement. Singly or in pairs. 4. Capsules. Found in some strains. 5. Spores. Nonsporing. 6. Motility. Motile by peritrichate flagella. 7. Staining. Stain readily with simple dyes; Cultural Characteristics 1. Grows readily on ordinary media. 2. Facultative anaerobes. 3. Optimum temperature 37°C, range 10-40°C. 4. Optimum pH 7.4-7.6. 5. In fluid media: (i) General turbidity in 24 hours. (ii) On further incubation, a deposit readily dispersible on shaking. 6. On solid media: (i) On nutrient agar, the colonies are round, smooth, raised, greyish, and semiopaque. (ii) On MacConkey's medium. Colonies bright pink. (iii) Growth is grossly inhibited on selective media, e.g., DCA or SS agar.
Biochemical Activity 1. Ferments glucose, lactose, mannitol, maltose with production of acid and gas. 2. Gelatin is not liquefied. 3. Indole is produced. 4. Methyl red positive. 5. Voges Proskauer test negative. 6. Citrate negative. 7. H2S not produced. Serology 1. Somatic O antigen. 2. Flagellar H antigen. 3. Surface K antigen - contributes to virulence by inhibiting phagocytosis.
Toxin Production
1. Endotoxin, associated with O antigen 2. Enterotoxin 3. Haemolysin
Pathogenicity
Generally a commensal in the intestine; produce: 1. Diarrhoea, particularly infantile diarrhoea 2. Cystitis 3. Pyelonephritis 4. Peritonitis 5. Wound infections 6. Abscesses.
SHIGELLA
Species 1. Sh. Shigae 2. Sh.flexneri 3. Sh. Boydii 4. Sh. sonnei.
Morphology
1. Shape. Rod shaped bacilli. 2. Size. 1.3 x 0.5µ 3. Arrangement. Single. 4. Motility. Non-motile. 5. Capsules. Noncapsulated. 6. Spores. Nonsporing. 7. Staining. Readily stained by simple dyes; Gram negative.
Cultural Characteristics
1. Grows readily on ordinary media.
2. Facultative anacrobe.
3. Optimum temperature 37°C, range 10-42°C.
4. Optimum pH 7.4.
5. On fluid media, (i) General turbidity in 24 hours. (ii) On further incubation, a deposit readily dispersible on shaking.
6. On solid media: (i) On nutrient agar, the colonies are small, circular, convex, smooth and translucent. (ii) On MacConkey's medium, colonies are colourless except Shigella sonnei which produces pale pink colonies. (iii) Growth is inhibited on Wilson and Blair bismuth sulphite medium.
Biochemical Activity
1. Carbohydrates. (i) Ferments glucose with acid production. (ii) Mannitol is fermented by some species; not fermented by Shigella shigae. (iii) Lactose not fermented (except Shigella sonnei).
2. Methyl red positive 3. Citrate negative. 4. H2S not produced.
Toxin Production
Shigella shigae produces an exotoxin; Shigella flexneri and Shigella sonnei produce endotoxin.
Pathogenicity
Shigellae produce bacillary dysentery.
SALMONELLA
Species 1. S.typhae 2. S. paratyphae A 3. S. paratyphae B 4. S. paratyphae C
Morphology
1. Shape. Rod shaped bacilli. 2. Size. 1.3 X 0.6µ 3. Motility. Motile by peritrichate flagella. 4. Capsules. Noncapsulated. 5. Spores. Nonsporing. 6. Staining. Readily stained by ordinary dyes; Gram negative.
Cultural Characteristics
1. Grows readily on ordinary media. 2. Facultative anaerobes. 3. Optimum temperature 37°C, range 15-40 °C 4. Optimum pH 7.4-7.6.
5. On fluid media 6. On solid media Biochemical Activity 1. Ferments glucose,
maltose, mannitol, dulcite Serology 1. Flagellar H
antigen. Heat labile protein, 2. Somatic O antigen. A
phospholipid-proteinpolysaccharide complex; present in the cell wall; weaker
than H antigen; heat stable. Pathogenicity 1. Enteric fever.
Diagnosis of Enteric Fever 1. Blood culture.
Posive in first week and mostly also second week.
(ii) A short round- bottomed tube (Felix tube) for O agglutination. Seven dilutions of
patient's serum are made in saline 1/10, 1/20, 1/40, 1/80, 1/160, 1/320,
1/640). O and H suspensions of Salmonella typhi (TO and TH respectively) and
H suspension of Salmonella paratyphi A and Salmonella paratyphi B (AH and BH respectively) are
used as antigens. Control tubes containing the antigen and normal saline are
set to check auto-agglutination. The tubes are incubated in a water bath at
37°C overnight Agglutination titres (highest dilution with agglutination) are
observed as in the table. The following factors should be taken into account in interpretation of Widal reaction: (i)
Agglutinins
remain in blood even after convalescence, therefore history of recent illness
should be taken. 5. Phage typing for tracing the source of infection and relationship between cases. Prophylaxis TAB vaccine 0.5 ml subcutaneously followed by 1ml subcutaneously after 7-10 days. PROTEUS Species 1. P. Vulgaris 2. P. mirabilis 3. P. morgagni 4. P. rettgefi. Morphology 2 Size. 0.5 x 1-3 µ 3. Motility. Actively motile by peritrichate flagella 4. Capsules. Non-capsulated. 5. Spores. Non-sporing. 6. Staining. Gram-negative. Cultural Characteristics 1. Grow readily on
ordinary media. 4. On solid media: Biochemical Activity Serology Pathogenicity PSEUDOMONAS Species 1. Ps. pyocyanea (Ps. aeniginosa) 2. Ps. mallei. Morphology 1. Shape. Rod shaped
bacilli. Cultural Characteristics 1. Grow readily on
ordinary media. Biochemical Activity 1. Liquefy gelatin.
Pathogenicity 4. Bronchopneumonia.
PASTEURELLA Species 3. Past. septica Morphology 1. Shape. Small
ovoid rods with rounded ends and convex sides. (ii) Staining is "bipolar" with intervening protoplasm less densely stained than the polar areas. Cultural Characteristics
5. On solid media: (i) On nutrient agar, the colonies
are small, tran5parent, delicate, colourless, granular and viscid. Later
these become opaque, greyish, irregular. Biochemical activity 1. Ferment glucose, maltose, rhamnose, glycerol manitol, after incubation for several days (i.e., weak activity) with acid production. 2. Litmus milk is not altered. 3. Gelatin not liquefied 4. Indole not produced 5. Broth rendered alkaline. Pathogenesity Pasteurella pestis causes plague in rats, which is conveyed to man through rat fleas Past. septica is occasionally isolated from respiratory tract infections and wounds inflicted by animal bites. BRUCELLA Species 1. Br. Abortus 2. Br. Melitensis 3. Br. suis, ,Morphology 1. Minute rods appearing as coccobacilli. 2. Size : 0.6-1.5 x 0.6 µ 3. Arrangement. Singly or in short chains. 4. Motility. Non-motile (except Br. bronchiseptica) 5. Spores. Non-sporing. 6. Capsules. Non-capsulated. 7.
Staining.
Cultural Characteristics 1. Grows readily on ordinary media but growth is not profuse. 2. Strict anaerobes. 3. Optimum temperature 37°C. 4. Optimum pH 7.2 7.4. 5. In fluid media: (i) After 24 hours,
slight turbidity. 6. On solid media: Biochemical Activity 1. Carbohydrates not
fermented. Pathogenicity Brucella melitensis. Malta kmediterranean or undulant) fever. Brucella abortus. Abortus fever. The disease is produced in goats, cattle, horses, sheeps and pigs from which these are conveyed to man. HAEMOPHILUS Species Haemophilus influenzae.
1. Shape. Minute
rods with considerable pleomorphism. Cultural Characteristics 1. Does not grow on ordinary media; grows on blood agar, still better on chocolate agar and Fild's medium. However, growth is never profuse. 2. Strict aerobe. 3. Optimum temperature 37°C. 4. On fluid media. Slight general turbidity; some strains give flocculent deposit with little turbidity. 5. On solid media. (i) Minute, smooth, transparent, circular colonies in 24 hours. (ii) On further incubation, growth is more marked and colonies become irregular in appearance.
Biochemical Activity
1. Ferments glucose, maltose, laevulose with acid production. 3. 2. Several strains produce indole.
Serology
The capsule of H. influenzae contains specific soluble substance (SSS). Six types (a to f) are identified.
Pathogenicity
Normal commensal in upper respiratory tract; may produce:
1. Bronchopneumonia 2. Antrum infections 3. Otitis media 4. Empyema 5. Endocarditis 6. Arthritis 7. Conjunctivitis 8. Meningitis.
BORDETELLA Species
1. Bord. Pertussis 2. Bord. Parapertussis 3. Bord bronchiseptica.
Morphology
1. Shape. Small ovoid cocco‑bacillus; on subculture becomes longer and threadlike. 2. Size. Average length 0.5 µ 3. Arrangement. In loose clumps with clear spaces in between (thumb print appearance). 4. Motility. Nonmotile. 5. Capsules. Capsulated. 6. Spores. Nonsporing. 7. Staining. Gram‑negative; shows bipolar metachromatic granules on staining with toluidine blue.
Cultural Characteristics 1. Does not grow on ordinary media on first isolation but after several subcultures it is able to grow on ordinary media. 2. Optimum temperature 37°C. 3. Strict aerobe 4. On fluid media, e.g., serum broth Uniform turbidity sometimes with slight deposit.
5. On solid media, e.g., blood agar (i) Colonies small and transparent in 24 hours. (ii) On further incubation, colonies become larger, greyish and opaque.
Commonly used medium is Bordet‑Gengou glycerine‑potato‑blood agar.
Biochemical Activity
Biochemically inactive; no action on carbohydrates and proteins.
Pathogenicity
Whooping cough.
CORYNEBACTE RIUM
Species 1. C. diphtheria 2. C. ulcerans 3. C hoffmanni 4. C. xerosis.
Morphology
1. Shape. Straight or slightly curved rods swollen at one end (clubbed). 2. Size. 3‑5 x 0.5µ 3. Arrangement. In pairs or small groups; the bacilli are arranged at angle to each other resembling letter L or 'V' (Chinese letter or cuneiform arrangement). 4. Motility. Nonmotile 5. Capsules. Noncapsulated 6. Spores. Nonsporing 7. Staining. Staining reaction uneven; Gram positive; decolourised easily. Granules retain the stain. Cultural Characteristics 1. Growth scant or ordinary media; more profuse on enriched media. Loffler's serum is the commonly used medium. 2. Optimum temperature 37°C, range 14-40°C. 3. Optimum pH 7.2. 5. On fluid media: On solid media: Classification of C. diphtheriae Depending upon the
appearance of colonies on chocolate tellurite agar, Corynebacterium diphtheria
is divided into three types: 2. Intermedius. Small, discrete, flat, black, granular colonies with a central papilla and slightly irregular edge. 3. Mitis. Convex, smooth, black, shining colonies. Biochemical Activity 1. Carbohydrates: 2. Proteins: Toxin Production Corynebacterium diphtheriae produces exotoxin. Almost all gravis and intermedius strains produce toxin which is not produced by a few mitis strains. However, the amount of toxin liberated is not related to virulence. Park 8 strain, which is relatively avirulent, produces abundant exotoxin and is universally employed as a source of exotoxin for laboratory purposes. Minimal lethal dose. The smallest amount of exotoxin killing a 250 gm guinea pig in four days. Minimal reacting dose. The smallest amount of exotoxin producing a definite reaction on intradermal inoculation into a guinea pig. Toxoid (Anatoxine). The toxicity of bacterial filtrate may be reduced by adding 0.2-0.4% formalin and incubating at 370C for 4-6 weeks. This modified toxin with intact antigenicity is termed toxoid or anatoxine. Pathogenicity Schick Test 1. Positive reaction,
Control forearm shows nothing; test forearm manifests a definite local
erythema in 24-48 hours, usually well marked by 4th day, then gradually fades
away leaving a brownish appearance. The negative reaction and pseudo-reaction indicate the person is immune to diphtheria. Positive and combined reaction suggest susceptibility and need for immunization. Immunization A. Active
immunization 8. Oral toxoid. Lozenges containing 1500 Lf doses of toxoid and 1500 units of hyaluronidase. Passive Immunization 500-1000 units of antidiphtheritic serum (ADS) subcutaneously. Serum Therapy In mild cases. 2,000-10,000 units. In severe cases. 10,000-50,000 units. The serum should be administered immediately on clinical diagnosis without awaiting laboratory report. General mode of administration is intramuscular. However, in severe cases intravenous administration should be made for quicker effect. MYCOBACTERIUM TUBERCULOSIS Morphology 1. Shape. Straight or slightly curved rods with rounded ends. 2. Size. 0.3-0.5 x 1.2 µ 3. Arrangement. Singly or in small groups. 4. Motility. Non-motile. 5. Capsules. Non-capsulated. 6. Spores. Non-sporing. 7. Staining.
Cultural Characteristics 1. Cold blooded types grow readily on ordinary media; human and bovine types are slow to grow even on special media; avian types are mid-way between these two. The commonly used medium is Dorset's egg. 2. Strict aerobe. 3.
Optimum
temperature. 4. Optimum pH. 7.0 - 7.6. 5.
On fluid media,
e.g., glycerine broth: 6. On solid media, e.g., Dorset's egg. Dry, friable, confluent colonies with granular or wrinkled surface. The human and bovine types grow slowly and may require 4-6 weeks for extensive growth. 7. On Dubos medium, small aggregated chains of bacilli known as sepentine cords. Biochemical Activity 1. Ferments glucose and maltose with acid production. 2. Presence of peroxidase and niacin production differentiate M. tuberculosis from other acid-fast bacilli. Serology There are three
serological types: The human, bovine and murine types are serologically homologous and differentiated on other grounds. Pathogenicity Tuberculosis. Immunity Infection-iminunity results from repeated doses of subclinical infections in person inhabiting endemic areas. This is evidenced by the following: 1. In endemic areas adults are tuberculin positive. 2. In adults the disease runs a chronic course whereas in children the course is more acute. 3. On post-mortem examination, the adults with no history of tuberculosis show localised foci of infection, particularly lymph nodes. 4. When tuberculous infection is introduced into new area both children and adults run a similar course, i.e., acute one. Koch's Phenomenon When, a healthy guinea
pig-is injected a small dose of tubercular bacilli, progressive lesions
develop and the animal dies ultimately. Allergic Tests 1. Von Pirquet Test. 2 drops
of undiluted tuberculin are placed on flexor aspect of the forearm about 10
cm apart; light scarification is carried out through the drops. A drop of 50%
glycerine is placed and scarified between the two tubreculin points as a
control.
Mantoux positive individuals are also vaccinated. mannitol, saccharose and starch with acid Immunization Active immunization is done with live attenuated vaccine called Bacille-Calmette-Guerin (BCG). The newborns are given this vaccination within a week. All the children and individuals below 15 years of age, who have not been previously immunized, are given B.C.G. vaccination without prior Mantoux testing. VIBRIO CHOLERAE Morphology 1. Shape. Short
curved rods with rounded or production; lactose
fermented late. Serology Vibrio cholerae prossesses somatic 0 antigen and flagellar H antigen. On the basis of wantigenicity vibrios are classified as under. A. Group A (cholera and cholera-like vibrios). 1. 0 subgroup I: (b) Haemolytic el tor vibrios: (iii) Hikojima. 7. Staining. Stained readily with aniline dyes; B. Group B (unrelated to cholera vibrios biocGram-negative. Cultural Characteristics 1. Grows readily on
ordinary media. Aerobic, but not very
strictly. 6. On solid media. Moist, translucent, greyish, round, and small (1-2 mm) colonies. Biochemical Activity 1. Indole produced rapidly. 4. Ammonia and H2S formed. 5.
Ferments glucose, laevulose, maltose,
Serology Vibrio cholera possesses somatic O antigen and flagellar H antigen. On the basis of antigenicity, vibrio are classified as under :-
Pathogenicity Cholera. ACTINOMYCES Species 1. A. bovis 2. A. madurae Morphology 1. Shape. Pleomorphic (i) In culture: Rods of
varying size with branching filaments, clubs and coccal forms. 2. Motility. Nonmotile.
Cultural Characteristics 1. Grow readily on ordinary media. Actinomyces bovis is anaerobic whereas 2. Actinomyces madurae (often put under separate genus as Nocardia madurae) is aerobic 3. Optimum temperature 37°C. 4. Optimum pH 7.2-7.6. 5. On fluid media. Delayed poor growth as white modular deposit resembling puff-balls, no turbidity or pellicle. 6. On solid media. Poor delayed growth as small, greyish-white, opaque, convex colonies. Pathogenicity Actinomyces bovis.
Actinomycosis. BACILLUS Species 1. B. anthracis 2. B. subtilis Morphology 1. Shape. Straight or slightly curved rods with truncated ends. 2. Size. 8 x 0.4 µ 3. Arrangement. Singly, in chains or in short chains. 4. Motility. Nonmotile. 5. Capsules. Capsulated; the entire chain may be enclosed in single capsule. 6. Spores. Not formed in animal tissue; in culture, spores are central or subterminal and do not buldge. 7. Staining. Gram-positive and non-acid-fast. Cultural Characteristics 1. Grow readily on
ordinary media. (ii) Later, flocculent deposit with clear supernatant fluid. 6. On solid
media: Biochemical Activity 1. Ferment glucose,
maltose, sucrose, and salicin with acid production. Pathogenicity Anthrax. CLOSTRIDIUM Species 1. Cl. Tetani 2. Cl. Welchii 3. Cl. Botulinum 4. Cl. butyricum. Morphology 1. Shape. Large, straight or slightly curved rods with rounded or truncated ends. 2. Size. 0.5 x 8 µ 3. Motility. Motile except Cl. welchii. 4. Capsules. present in Cl. welchii and Cl. butyricum. 5. Spores. Wider than bacillus; commonly central or subterminal; terminal in Cl. tetani. 6. Staining. Stain readily with ordinary dyes; Gram-positive; spores are stained by special stains only. Cultural Characteristics 1. Grow under
strictly anaerobic conditions. (i) In broth (under
anaerobic condition), turbidity with a moderate granular or powdery deposit.
5. On solid media Poor and slow growth with small, effuse, and irregular colonies. On blood agar, some species show haemolysis. Biochemical Activity 1. Saccharolytic activity with gas (CO2 and hydrogen) production is exhibited by Cl. welchii, but not by Cl. tetani. Glucose, maltose, lactose and sucrose are fermented. 2. Proteolytic activity is well marked in a botulinum which acts on gelatin, casein, serum, and fibrin; meat is digested and blackened. It is less marked in Cl. welchii and C1. tetani; these liquefy gelatin but do not digest serum, fibrin or meat. 3. Litmus milk changes (i) Proteolytic members produce peptonization and digestion. (ii) Saccharolytic
members produce acid, gas and clot. Toxin Production Produce exotoxin. Pathogenicity C1. tetani. Tetanus. C1. welchii. Gas gangrene. C1. botulinum. Botulism. SPIROCHAETES Spirochaetes are elongated, motile, flexible bacteria which are twisted spirally round the long axis. A characteristic property of spirochaetes is their motility without the presence of flagella. This is due to varying numbers of fine fibrils between the cell wall and cytoplasmic membrane, anchored at the two poles of bacterial cell. Motility is serpentlike, and of three types: 1. Flexion and extension 2. Cork-screw like rotary movements 3. Translatory motion. Spirochetes are divided in two families: A. Family spirochaetaceae
(saprophytes): B. Family
treponemataceae: BORRELIA Species 1. Borr. Recurrentis 2. Borr. vincentii. Morphology 1. Shape. Large, refractile, with irregular, wide, open coils. 2. Size. 10-30 x 0.3-7 µ
4. Staining. Readily stained by ordinary dyes; Gram-negative. Cultural Characteristics Difficult to grow; the usual media are: 1. Ascitic fluid containing rabbit kidney (Noguchi's medium). 2. Chorioallantoic membrane of chick embryos. 3. Intraperiteneal inoculation in mice or rats. Pathogenicity Borrelia recurrentis. Relapsing fever. Borrelia vincentii. Vincent's angina. LEPTOSPIRA Species Lept. icterohaemorrhogiae. Morphology 1. Shape. Multicoiled with hooked ends resembling umbrella handles. 2. Size. 6-20 x 0.1 µ 3. Motility. Motile. 4. Staining._ Not stained by ordinary dyes; may be stained by Giemsa stain by silver impregnation methods. Cultural Characteristics 1. Optimum temperature 30°C. 2. Optimum pH 7.2-7.5. 3. Media used. (i) Semi-solid blood agar. (ii) Chorio-allantoic membrane of chick embryos. (iii) Inoculation in guinea pigs. Pathogenicity Weil’s disease. les TREPONEMA Species 1. T. pallidum 2. T. pertenue 3. T. carateum. Morphology 1. Shape. Thin, delicate spirochaetes with tapering ends. 2. Size. 4-14 x 0.1-0.2 µ 3. Motility. Motile. 4.
Staining.
(ii) Light rose red with Giemsa stain. (iii) Negative stain with India ink or Congo-red
Cultural Characteristics Pathogenicity Standard Tests for Syphilis 1. Wassermann Reaction
2. Patient's serum 3. Complement 6. Saline. Technique
Table : Wassermann Reaction Interpretation 2. Kahn Test Reagent Required 1. Antigen. Alcoholic extract of ether-insoluble lipoids of beef heart. 2. Patient's serum
inactivated by heating at 560C 3. Saline.
Technique
Table : Kahn Test The test is carried out in
small special tubes. 4 such tubes are arranged in a rack and proceeded
as, in the table Interpretation A definite precipitate suspended in a clear medium is considered a complete reaction and is read four plus. Proportionally weaker reactions are read three, two and one plus, respectively. The final result in each test is the average finding of the three tubes. Thus, if the precipitation reaction is four plus in each of the three tubes, the final result is four plus. If the reaction is -, +++, ++++, the final result is two plus. Tube 4 acts as a control and should show uniform opalescence. 3. VDRL Test 0.05 ml of inactivated
serum (heated at 56°C for 30 minutes) is taken on a special slide with
depression. One drop of freshly prepared antigen is added by means of a
syringe delivering 50 drops per ml. The slide is rotated at 180
rotations/minute in a special VDRL rotator for 4 minutes. It is then examined
under low power of the microscope. Uniform distribution -of crystals in the
drop indicates negative reaction whereas formation of clumps indicates
positive reaction. RICKETTSIAE Morphology 1. Shape. Pleomorphic cocco-bacilli. 2. Size. 0.3-0.6 x 0.8-2.0µ 3. Mostly nonmotile.
(i) Not well-stained by
Gram stain; Gram negative.
Cultural Characteristics 1. Do not grow on ordinary media. 2. Readily cultivated in yolk sac of
developing chick embryos. Weil-Felix Reaction This is employed for the diagnosis of some reckettsial diseases. The reaction is an agglutination by the serum of typhus patients of strain of proteus, mostly strain 'OX 19'. Titres as high as 1/50,000 are obtained during febrile stages. Pathogenicity of Rickettsiae
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Chapter 15 : Virology General
Properties 4. Viruses have host
specificity. They attack Structure specific cells in particular hosts. Morphology Size Viruses are ultramicroscopic organisms not visible under ordinary optical microscope. The size is expressed in millimicrons (nm) which is 1/1,000 of a micron (µ) or 1/1,000,000 of a millimetre (mm). The range is 20-300 nm. Virion or elementary body is the infectious virus particle. All the sizes of viruses refer to the size of virion. The size of a virion is determined by the following methods: 1. By filtration through
collodion membrane of varying
grades of porosity. Structure The virus particle or virion consists of a central core of nucleic acid surrounded by protein coat called capsid. Capsid is composed of polypeptide molecules arranged symmetrically to form a shell around the nucleic acid core. The capsid protects the core from inactivation by nucleases and other agents. When progeny of virions is released by budding, the virion is covered by peplomer, a covering derived from the host cell membrane and lipoprotein in nature. The protein component is virus-coded whereas lipid component is largely of host cell origin A capsid may be polygonal (icosahedron) with corners (vertices) and sides (facets); or it may be spiral (helical). Viruses contain only one type of nucleic acid, MMtzC'_WII acid (RNA) or deoxyribonucleic acid The extracted nucleic acid is at times of infecting the host cell. Cultivation Viruses cannot grow on acellular media and special methods of cultivation. The media employed are given below:-
Inclusion Bodies Inclusion bodies are
structures with specific shape, size, location and staining properties
present in the virus infected cells, and visualised under optical Examples 1. Negri bodies.
Intracytoplasmic eosinophilic inclusion bodies of rabies virus in the brain
cells of animals. 3. Bollinger bodies. Large
inclusion bodies of fowl Pox virus. 5. Intranuclear inclusion bodies: (i) Cowdry typeA. Herpes
virus, yellow fever. Bacteriophages are the viruses which infect bac- Classification A. DNA viruses: 2. Adenovirus
Pox-viruses: (i), Variola (ii) Vaccinia. 5. Parvovirus. B. RNA viruses: 1. Picorna virus: 2. Togavirus C. Unclassified viruses: BACTERIOPHAGE Bacteriophages are the viruses which infect bacteria. Thus these are the viruses which can be grown in laboratory media along with corresponding bacteria. The bacteriophages have specificity for bacterial species and are thus valuable in diagnosis, the process being called phage-typing. Properties 1. Bacteriophage acts on
multiplying organisms. It clears the young broth cultures either temporarily
or permanently. On solid media clear zones are formed. Application (i) Colicins for Escherichia coli. (ii) Pyocins for
Pseudomonas pyocyanea. 3. As these are cultivable on laboratory media, they provide a useful material for study of properties of viruses. POX-VIRUSES The causative agent of classical smallpox is Variola major, that of a milder form of smallpox (alastrim) is Variola minor. The two viruses are antigenically identical and appear to be stable variants of the same virus. The virus from a case of smallpox never produces alastrim and vice versa. Vaccinia virus is not found in nature and does not produce any disease. The cowpox virus used by Jenner for vaccination underwent mutation and the new virus named Vaccinia proved more useful in vaccination. The present stalks of vaccinia virus throughout the world, are the progeny of the original modified cowpox virus. Vaccinia is thus an artificial virus, very much similar in properties with variola virus. Structure T he virion is a large one (size 0.125 - 0.175µ), brick shaped. The core made up of DNA is biconcave, surrounded by a double layered membrane. The virion or elementary body is termed Paschen body. Resistance The virus is resistant to glycerine, phenol, ether and freezing. It is destroyed by heating over 55°C and by potassium permanganate, formalin and oxidizing disinfectants. Serology Pox viruses bear the following antigens: 1. LS antigen comprising two antigens heat labile L and heat stable S. 2. Agglutinogen.
3. Nucleoprotein (NP) antigen. 4. Haemagglutination 5. Protective antigen
Nucleoprotein antigen is common to all pox viruses whereas other antigens are subgroup specific.
Inclusion Bodies Inclusion bodies of pox-virus are known as Guarnieri bodies. These are small, multiple and intracytoplasmic bodies present in the epithelial cells of the lesion. Inclusion bodies are aggregations of virus particles in a matrix. Cultivation 1.
On
chorio-aflantoic membrane of 11-13 days old chick embros; pocks are produced
in 2-3 days. The ceiling temperature
beyond which pocks fail a develop also varies: 2.
Tissue culture
in: 3. Animal inoculation. In monkeys, calves, sheep, rabbits. Paul's Test Scarification of rabbit cornea with variola virus leads to keratitis and sections of the cornea show typical Guarnieri bodies. Vaccination Routine vaccination against smallpox was stopped in India after irradication of the disease. Primary vaccination was given within a week after birth followed by secondary vaccination every five years. In vaccination, live attenuated virus lymph is placed on cleansed skin and light scarification carried out. A local vesicular lesion develops in 3-5 days which develops into a pustule and ultimately dries off. HERPES VIRUSES Herpes Simplex Virus Properties 1. Resistant to 50% glycerine and freezing 2. Readily destroyed by heating over 50°C 3. Relatively large, 100-150 nm 4. Can be cultured in vitro in the presence of living cells. Pathogenecity The virus infects only man. A. Primary lesions:
B. Secondary lesions:
Varicella Virus Varicella virus produces two diseases in man viz. varicella (Chicken pox) and Herpes zoster. Chicken pox is the result of primary infection whereas herpes zoster is reactivation of old silent infection. Virus from a case of herpes zoster may produce chickenpox but not the reverse. Properties 1. Resistant to 50% glycerine and freezing 2. Readily destroyed by heating over 55°C 3. Relatively large, 100-150 nm 4. Can be grown in
cultures of: POLIO-VIRUS It belongs to subgroup Enteroviruses of RNA virus group Picorna viruses. Structure 1. Among the smallest viruses, virion size about 27 nm 2. Capsid is polygonal (icosahedral) 3. Can be crystallized. Resistance 1. , Resistant to freezing, drying, pure glycerine and 0.5% phenol 2. Readily destroyed by heat over 45°C and oxidizing agents. Serology 2. Type 2 or Lansing type 3. Type 3 or Leon type. Brunhilde type is the commonest and associated with most of the epidemics. Inclusion Bodies Inclusion bodies are intranuclear and of Cowdry type B. Cultivation Grows on primary monkey kidney cultures.
Immunization 1. Salk vaccine
2. Sabin vaccine
INFLUENZA-VIRUS Influenza virus belongs to group Orthomyxovirus of the RNA viruses. - Structure 1. The virion is
relatively large, 100 nm 3. The virus is covered with a double layer envelope (peplomer) consisting of inner virus protein layer and outer lipid layer of host cell origin. Resistance 1. Resistant to drying and fruezing. 2. Killed by heating at 50°C for 30 minutes inactivated by chemicals like ether, phenol and formalin. Serology 1. RNP antigen (S antigen). Type specific intemal antigen of types A, B, and C. 2. V antigen. Surface antigen comprising two components :- (i) Haemagglutinin -strain specific (ii) Neuraminidase -strain specific. Serological diagnosis is by complement fixation and haemagglutination. Cultivation 1. Tissue cultures 2. Chorio-allantoic membrane of chick embryos. ARBOVIRUSES These are RNA viruses transmitted biologically by the insects. Properties 1. Small spherical viruses, size 20-60 nm. 2. Possess lipid envelope making them susceptible to bile salts and ether. 3. Inactivated at room temperature; with-stand freezing. 4. Multiply in arthropods (insects). 5. Can be grown in tissue cultures of (i) Chick embryo fibroblasts. (ii) (ii) Insect tissues. 6. Agglutinate red cells of goose and day-old chick. 7. Possess three antigens: (i) Haemagglutinins (ii) Complement fixing antigen (iii) Neutralizing antigen. Classification A. Group A 1. Encephalitis viruses: (i) Eastern equine encephalitis (EEE) virus (ii) Western equine encephalitis
(WEE) virus B. Group B 1. Mosquito-borne: (i) St. Louis encephalitis virus (ii) Ilheus virus (iii)West Nile virus (iv) Murray Valley encephalitis virus (v) Japanese B encephalitis virus. b. Yellow fever virus c. Dengue virus. 2. Tick-borne: b. Haemorrhagic fever
viruses: RABIES VIRUS Rabies virus belongs to group Rhabdovirus of RNA viruses. Properties 1. Relatively large virus, virion size 100-150 nm. 2. Virion is surrounded by double layered lipoprotein envelope; the protein is virus coded and lipid is of host cell origin. 3. It resists glycerine and low temperatures. 4. Inactivated by drying, 1% phenol, oxidizing agents, ether, and heating over 45°C. 5. Grown on tissue cultures and yolk sac of chick embryos. 6. Inclusion bodies, known
as Negri bodies are eosinophilic and present in cytoplasm. Prophylaxis The types of vaccines are: 1. Pasteur's vaccine. The spinal cord of rabbits 3. inoculated with fixed virus is dried over potassium hydroxide. Saline suspensions of cord are prepared when required. Most attenuated virus is one dried for the longest period (14 days) and the least attenuated is the one dried for 5 days. Serial injections are given with decreasing attenuations. 2. Hogye's vaccine Active
virus diluted to 1/10,000 is used for initial injections, the dilution is
gradually reduced. 5. Remlinger's vaccine. Virus attenuated by ether. |
|||||||||||||||||||||||||||
|
Chapter 16 : Parasitology CLASSIFICATION OF PROTOZOA Protozoa has 4 classes:
ENTAMOEBA HISTOLYTICA Entamoeba histolytica, occurs as a pathogenic parasite in man. Habitat The vegetative
(unencystic) occur in: The cysts are formed in the large intestine; neither formed in liver nor outside the body. Morphology
1. ectoplasm 2. endoplasm 3. nucleus 4. karyosome 5. vacuoles 6. ingested red blood cells. 4.
Spherical nucleus bounded by a thin limiting membrane; dividing organism may show 2 nuclei.
7. Endoplasm contains vacuoles, with food particles erythrocytes, portions of leucocytes, and occasionally bacteria. 8. Movement is by temporary prolongations of cytoplasm, pseudopodia. B. Encysted form: 1. Cysts are round
or oval, of pearly colour with a cyst wall.
3. Four or fewer nuclei. 4. Newly formed cyst has single nucleus, glycogen mass and one or usually two characteristic chromidial bars or chromatoid bodies. Pathogenicity Entamoeba histolytica is incapable of survival by itself and derives its metabolic requirements from bacteria. Amoebiasis is characterised by penetration of host tissues by entamoeba, necrosis of tissue cells and absence of inflammatory reaction. Lesions are most commonly found in the caecum, ascending colon, sigrnoid and rectum, appearing as flask-shaped ulcers. Clinical Types of Amoebiasis 1. Asymptornatic cyst passers (commonest) 2. Amoebic diarrhoea 3. Amoebic dysentery 4. Amoebic appedicitis 5. Amoebic typhlitis (inflammation of caecum) 6. Amoebic granuloma (tescmbling carcinoma) 7. Amoebic hepatitis 8. Amoebic abscess in liver, lung, brain and other organs 9. Amoebic perianal dermatitis. Diagnosis 1. Stool Examination:
2. Examination of proctoscopic aspirate and biopsy scraping. 3. Complement fixation test. 4. Haemagglutination reaction. Chemotherapy 1. Alkaloids of ipecac, such as emetine hydrochloride, 65 mg daily subcutaneously for 10 days, effective against intestinal as well as extraintestinal amoebiasis. 2. Halogenated quinolines, such as iodochlorohydroxyquinoline, 600 mg thrice a day for 3 weeks; effective against intestinal amoebiasis. 3. Aminoquinolines, such as chloroquine phosphate 1 g daily for 2 days, then 0.5g daily for 14-21 days, effective against intestinal as well as extraintestinal amoebiasis. 4. Arsenicals, such as glycobiarsol 0.5 g thrice a day for 7 days; effective against intestinal amoebiasis. 5. Diloxanide furoate (Furamide),0.5 g thrice daily for 10 days; effective against intestinal as well as extraintestinal amoebiasis. 6. Metronidazole, 2.4 g
daily for three days, or tinidazole 2.0 g daily for three days; effective
against intestinal and extraintestinal amoebiasis.
Chart : Life cycle of Entamoeba histolytica GIARDIA INTESTINALIS Habitat 1. Upper part of small intestine 2. Cysts present in faeces. Morphology A. Vegetative form: 1. Shaped like badminton racquet, when flat and like half-pear when viewed from side; one surface (dorsal) is convex and the other (ventral) concave.
2. Sucking disc, indented posteriorly, with a raised circumference. 3. Two nuclei, one on each side of the body. 4. Eight flagella, out of which one arises from the region of sucking disc. B. Cystic form: 1. Oval in shape.
Life Cycle 1. Multiply in the
intcstine of man by longitudinal division into two; vegetative forms do not
survive in faeces. Pathogenicity 1. Diarrhoea.
Chemotherapy 1. Atabrine 100 mg
thrice a day for 5 days. TRICHOMONAS VAGINALIS Habitat 1. Female genital
tract. Morphology 1. Occur only in
vegetative form, trophozoite, no encysted form.
6. Undulating membrane, formed by a thick flagellum passing backward and coming out free at posterior end; supported at the base by rod shaped costa. 7. Exostyle runs down the middle of the cell and ends in pointed tail like extremity. Pathogenicity Trichomonilial vaginits.
Chemotherapy
TRYPANOSOMA GAMBIENSE Habitat Morphology 2. Length 8-30µ;
longer organisms have long flagellum, shorter ones have none or small flagellum. 4. Near the posterior end lies kinetoplast from which flagellum arises. 5. Well-developed undulating membrane. 6. Cytoplasm contains granules and vacuoles of varying sizes.
Life cycle
Pathogenicity Sleeping sickness (in fact a stage of the disease Trypanosomiasis) in Tropical Africa.
Diagnosis
5.Animal inoculation of blood, lymph node juice or
cerebrospinal fluid in guinea pigs, rats or mice. Chemotherapy |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
TRYPANOSONIA CRUZI Habitat 1. In the blood stream of man, cats, and armadillos. 2. Leishmanioid forms in tissues of man and animals 3. Crithridia and metacyclic forms in the gut of bugs (Triatoma negista, T. infestans) Morphology A. In blood smear 5. Undulating membrane not much folded.
Life cycle
Pathogenecity Chaga's disease in South America. Diagnosis 1. Peripheral blood smear 2. Animal inoculation. LEISHMANIA Species 1. Leish. Donovani 2. Leish. Tropica 3. Leish. brasiliensis. Habitat 1. Cells of
reticulo-endothelial system in the spleen, liver and bone marrow. Morphology A. Leishmania form in man:
Left: Mass of parasites in a macrophage Right: Leptomonas form. B. Leptomonas form in sandfly 2. Free flagellum without undulating membrane 3. Elongated body, 10-20µ long 5. Kinetoplast anterior. Life Cycle
Pathogenicity 1. Kala-azar, caused by
Leish donovani; characterized by irregular prolonged fever, chronicity,
splenomegaly, at times hepatomegaly, emaciation, anaemia, leucopenia,
hyperglobulinuria, and skin pigmentation. Diagnosis 4. Chopra's antimony test. Add 2 drops of 4% urea stibamine solution to 1 ml of diluted serum. (in normal saline 1: 10). Immediate flocculation and turbidity indicate positive test. 5. Complement fixation test. 6. Blood culture on NNN blood agar medium. 7. Skin test. Chemotherapy 1. Pentavalent antimony
preparations, such as sodium stibogluconate (Pentostam.) 0.6-0.8 g daily
intravenously for 14 days. MALARIAL PARASITE Species 1. Plasmodium vivax Benign tertian malaria. 2. Plasmodium malariae. Quartan malaria. 3. Plasmodium ovale. Ovale tertian malaria. 4. Plasmodium falciparum. Malignant tertian malaria Habitat 1. Red blood cells
of man. Morphology The distinguishing features of various species are in the table.
Table : Comparison of four Species of Plasmodium
1. Asexual forms A. Small trophozoite (Ring form) The rings (or signet rings) are stout, large, measuring about 1/3 of the diameter of red cell. B. Large trophozoite (pre-schizont): 1. Irregular in shape. 2. Delicate. 3. Many pseudopodial processes; active amoeboid movements. 4. No vacuolated area. 5. Fine grains of brown pigment, haematin. C. Schizonts. 1. Size equals red cell; parasitised red cell becomes distended and larger. 2. Nucleus divided into several segments, each surrounded by cytoplasm; these segments along with cytoplasm are called merozoites. The pigment spot remain separate from merozoites as residual body. II. Sexual forms (Gametocytes): 1. Size equals red cell; no segmentation. 2. Male gametocyte or microgametocyte has pale blue cytoplasm, pigment distributed and nucleus diffuse. 3. Female gametocyte or macrugametocyte has dark blue cytoplasm, pigment ' collected together around compact nucleus. Modes of Infection 1. Bite of infected female anopheles mosquito. 2. Transplacental (congenital malaria). 3. Blood transfusion. Pathogenicity 1. Cold stage. It lasts about half an hour. The patient feels intense cold and shivers from head to foot; his teeth chatter and he covers himself under blankets. He has severe headaches and often troublesome vomiting. The temperature goes on rising.
2. Hot stage. It lasts 1-6 hours. The patient feels burning hot and may be delerious. Vomiting often continues to this stage. The face is flushed, and the skin dry and burning. The temperature rises to 39-41°C. 3.
Sweating stage.
Profuse perspiration starts. Types of Malaria 1. Benign tertian malaria (P. vivax). There is spontaneous remission and a greater tendency to relapse. 2. Quartan malaria (P. malariae) The attacks are of short duration and occur every fourth day. Nephritis is a common complication. 3.
Malignant tertian
malaria (P. falcipaum). The fever is rather remittent and tertian periodicity
of the infection is indicated by exacerbation of continuous fever.
Prostration is more marked and the tendency to delirium greater. Dangerous
severe forms of falciparum malaria are termed pernicious malaria, which may
be of the following types: (d) Gastric malaria. Characterised by persistent vomiting. (e) Dysenteric malaria. Characterised by bloody diarrhoea due to excessive capillary thrombosis in the intestinal walls. Laboratory Diagnosis 1. Blood films. Thick blood films are more helpful than thin Wood films. The films are stained with Field's rapid method immediately on being apparently dry. The stain consists of two solutions A and B: (a) Solution
A: (b) Solution B: Staining Procedure (a) Dip film for one second in solution A (b) Rinse in water (c) Dip for one second in solution B (d) Rinse in water. In addition to various stages of malarial parasite, the film may also reveal leucocytes containing ingested malarial pigment. 2. Sternal puncture. 7. Immunofluoroscence test. A patient with malaria may give positive Wassermann and Kahn reactions. Chemotherapy 1. Suppressive cure: (a) Chloroquin phosphate (Melubrin) 1.0 g single dose. (b) Amodiaquin (Camoquin) 0.6 g single dose. 2. Radical cure. Primaquin 15 mg once daily for 2 weeks, ineffective in active phase. 3. Chemoprophylaxis. Chloroquin phosphate 0.5 g, amodiaquin 0.3 g or pyrimethamine (Daraprim) 25 mg orally once a week. CLASSIFICATION OF HELMINTHS I. Phylum Platyhelminthes A. Class Cestoda: B. Class Trematoda:
II. Phylum Nemathelminthes 1. Ascaris lumbaricoides 6. Ankylostoma duodenale 7. Nectar americanas 8. Wuchereria bancrofti 9. Loa loa 10. Dipetalonema perstans 11. Filaria ozzardi DIBOTHRIOCEPHALUS LATUS Habitat 1. Adult in the intestine of man, cats, dogs, beers 2. Eggs in faeces 3. Larva first in cyclops, then in fresh water fish. Morphology (a) Worm 3-4 metres in length, 1-2 cms in breadth. Number of segments variable; may exceed 4,000. Segments are broader than long. Yellowish grey in colour.
Scolex showing sucking groove (bothrium)
Head (Scolex): (c) Genitalpores: (d) Testes: (e) Uterus: 1. Rosette shaped.
(f) Eggs: 1. Operculated.
(g) Hexacanth-embryo
(oncosphere): Llfe Cycle
Chart : Life cycle of
Dibothriocephalus latus Pathogenicity 1. Megaloblastic anaemia (vitamin B12
deficiency). 3. Occasionally, jaundice 4. Low erythrocyte count; nucleated cells; poikilocytosis. 5. Eosinophilia. 6. Colour index >
1 (as in pernicious anaemia). Diagnosis Stool Examination for: 1. Eggs. Chemotherapy
1. Globular. TAENIA SOLIUM Habitat 1. Adult worms in
small intestine of man. Morphology (a)
Worm: 2. 800-900 segments.
(b) Head (Scolex) 1. Globular 2. 0.6-1.0 mm in diameter .
3. Rostellum has a double crown of about 28 hooks. 4. Large hooks (160-180µ) alternate with small hooks (110-140µ).
(c) Genital pores 1. Irregularly alternate. 3. Thick, brown, radially striated embryophore. 4. Minute hexacanth embryo measuring 14 µ. (d) Uterus 1. Consists of a median longitudinal stem. 2. 8-10 lateral, compound branches on each side.
(e) Eggs: 3. Thick, brown, radially striatedembryophore. 4. Minute hexacanth embryo measuring 14µ
Fig 16.16 Life cycle of Taenia solium Pathogenicity A. Adult worm: 2. Diarrhoea or constipation. 3. Vomiting. 4. Anorexia. B. Cysticercus
cellulosae Diagnosis A. Adult worm:
B. Cysticercus
cellulosae: Chemotherapy As in Dibothriocephalus latus Habitat TAENIA SAGINATA Habitat 1. Adult worms in small intestine of man. 2. Eggs in human faeces. 3. Larvae in muscles of cattle. Morphology
1. 3-4 metres in length, 1-1.4 cm in breadth. 2. Over 1,000 segments. 4. Scolex does not bear hooks. 5. Uterus consists of a central longitudinal stem which bears 18-30 compound lateral branches on each side. 6. Eggs as in Taenia solium.
Fig. 16.18 Ovum of Taenia saginata. Life cycle
Chart : Life cycle of Taenia saginata
Pathogenicity and Diagnosis As in Taenia solium; the scolex has no hooks; larval stage not found in man. Chemotherapy TAENIA GRANULOSA
Habitat 1.
Adult worm in
intestine of dogs, jackals, wolves foxes, cats (not in man). 2. Eggs in faecee of above-mentioned animals. 3. Larval form (hydatid cyst) in sheep cattle, horses and man Morphology I. Size 4 mm x O.5mm
Hydalid cyst Life Cycle
Chart : Life cycle of Taenia granulosa Pathogenecity Hydatid cyst Diagnosis 1. Eosinophils 30-35%. 2.
Precipitin
reaction. Mix equal parts of patient's serum and preserved hydatid fluid and incubate at 37°C for one hour.
Observe for flocculation.
If it occurs within 36 hours, it suggests hydatid cyst. Negative test however, is not
conclusive. HYMENOLEPIS NANA Habitat 1. Adult worms in small intestine of man, rats and mice. 2. Eggs in faeces. 3. Larvae in intestinal villi. Morpholog y 2. 2-3 cm in length, 0.6 mm in breadth.
3. Over a hundred segments; broader than long.
4. Genital pores are
unilateral; situated on left anterior corner in each segment.
11. Outside the embryophore is a thick layer of semi-fluid substance, surrounded by a thin egg shell. Life Cycle
Chart : Life cycle of Hymenolepsis nana Pathogenicity Usually symptomless; may produce: 1. Diarrhoea with mucus and tenesmus. 2. Vertigo. 3. Epileptic convulsion. Diagnosis Ova in faeces. Chemotherapy As in Dibothriocephalus latus SCHISTOSOMA HAEMATOBIUM 1. Adult worms in
portal vein and its radicles, and especially the vesical plexus of man.
Morphology A. In both sexes B. Male worm 1. Colourless; 1 cm
in length; lateral margins
are covered ventrally. 3. Gynaecophoric canal
extends from the posterior extremity of the body to ventral sucker.
8.
A vas efferens
arises from each testis; these four unite to form vas deferens, which dilates
into a seminal vesicle from which it continues to genital pore. 1. Cylinderical, thread-like, dark coloured; extremities pointed. 2. 2 cms in length (longer than male). 3. Skin smooth; not tuberculated but minute spines may occur on the suckers. 4. The suckers are smaller than in male worm and almost equal in size. 5. Ovary is a small elongated organ situated in the posterior half of the body. 6. Oviduct arises from posterior extremity of ovary and immediately turns and runs anteriorly. 7. Vitelline glands occupy the posterior fourth of the worm, extending from a point immediately behind the ovary, to the posterior extremity of the body. 8. From the anterior extremity of vitelline glands, the vitelline duct arises, runs parallel with the oviduct and unites with it just in front of ovary. 9. Shell glands surround the junction of oviduct with vitelline duct.
10.The common duct dilates into an ootype, then narrows and runs forward
as uterus to genital pore. D. Eggs 1. Compact elongated spindles 2. Dilated in the middle. 3. 140µ x 50µ in size 4. Short, stout, terminal spine at one pole. E. Miracidium F. Sporocyst G. Cercaria
Life cycle
Chart : Life cycle of Schistosoma haematobium Pathogenicity 1. Sandypatch appearance in bladder walls. 2. Endophlebitis blocking the lumen of radicles of portal vein. 3. Papillomata containing numerous eggs on walls of bladder; ulceration and haemorrhage; may become malignant. 4. Liver and spleen enlarged. 5. Blood and mucus in stools. Diagnosis Chemotherapy CHLONORCHIS SINENSIS Habitat Morphology 1. The body is delicate, nearly transparent, brownish-red and, when young, covered with minute spines.
Life Cycle
Chart : Clonorchis sinenses Pathogenicity Diagnosis Habitat FASCIOLA HEPATICA Habitat 1. Adult worms in bile ducts of sheeps, goats, cattle, horses, pigs, and rarely of man. 2. Eggs in faeces 3. Larval stages viz. sporocysts, rediae, cercariae in fresh water mollusk, Limnoea truncatula. 4. Infective encysted cercariae found on blades
Morphology 1. 3.5 cm X 1.2 cms;
7. Two testes, one
posterior to other in immature worm but overlapping in adult worm;
extensively branched. 12. The uterus is short, rosette-shaped, situated immediately behind the ventral sucker; opens close to vas deferens, immediately in front of ventral sucker. 13. Eggs opperculated, 140 µ x 80 µ, contain a large refractile, fertilized, unsegmented ovum which lies in a mass of yolk cells. Life Cycle
Chart : Life cycle of Fasciola hepatica Pathogenicity 1. Adenoinata 2. Obstructive jaundice 3. Liver cirrhosis 4. Worm abscesses in different parts of body. Chemotherapy Emetine 30 mg daily by intramuscular route for 18 days. PARAGONIMUS WESTERMANII Habitat 1. Adults in the lung,
pleura, bronchi, occasionally in liver, spleen and other organs of man, dog,
cat tiger, wolf and pig. Morphology 1. Fleshy reddish brown, resembling one half of a pea. 2. 1.2 cm long, 6 mm broad, 5 mm, thick.
.
3. Genital pore in
midline just behind ventral sucker. Life Cycle
Chart : Life cycle of Paragonimus westermani Pathogenicity 1. Cysts resembling
tubercle nodules. Diagnosis Eggs in sputum of faeces. Chemotherapy Bithional 2.0 g alternate days for 3-4 weeks. ASCARIS LUMBRICOIDES Habitat 2. Eggs in faeces. 3. Infective larvae in eggs in soil, water or green vegetables. Morphology (b) Male worm: (c) Female wonn:
(d) Eggs: 2. 60µ x 45µ
3. Egg shell colourless and extremely resistant surrounded by a stout albuminous coat whose surface is thrown into rugosities or mammillations, which stain brown with faecal matter. 4. Within the egg shell is a very delicate vitelline envelope, still more resistant than egg shell making the eggs viable for several years. Life Cycle
Chart : Life cycle of Ascaris lumbaricoides Pathogenicity 1. Haemorrhages (minute) in intestine, liver, lungs. 2. Lobar pneumonia. 3. Toxaemia. 4. Peritonitis. Diagnosis Eggs in faeces. Chemotherapy 1. Piperazine (Antepar) 3 g single dose. 2. Tetramisole (Decaris) 150 mg single dose. 3. Thiabendazole (Mintezol) 1.5 g after evening meal, repeated after next morning meal. ENTEROBIUS VERMICULARIS Habitat 1. Young and mature
adult worms in small intes Morphology
.
(a) Male worm: (b) Female worm: (c) Eggs: 1. Coiourless,
asymmetrical, slightly flattened on one side.
Life Cycle
Chart : Life cycle of Enterobius vermicularis Pathogenicity 1. Perianal itching. 2. Acute appendicitis. Diagnosis 1. Adult worms in faeces. 2. Eggs on scrappings from perianal skin. Chemotherapy 1. Piperazine (Antepar) 1.5 g daily x 7 days. 2. Thiabendazole (Mintezol) 1.5 g after evening meal repeated after 24 hours. 3. Tetramisole (Decaris) 150 mg repeated after 48 hours.. 4. Pyrantel pamoate (Pyranthel) 11 mg per kg body weight to be repeated after 2 weeks.
Habitat 1. Primary infection with males and females in the lungs. 2. Secondary infection with females, rarely males, in intestine, particularly jejunum. 3. Larvae (not eggs) passed in human faeces. 4. Infective larvae on woodwork of latrines, soil and water; may occur in sputum. Morphology (a) Female worm (parasitic
form)
3. Vulva opens at the junction of middle and posterior
third of the body. 4. Vulva lies near middle of the body. (c) Male worm 3. Tail curved centrally 4. Two minute, brown
curved spicules each measuring 40 µ (d) Larvae Life cycle
Chart : Life cycle of Strongyloides stercoralis Pathogenicity 1. Acute intractable diarrhoea
with blood and mucus. Diagnosis 2. Filariform larvae in sputum. Chemotherapy TRICHURIS TRICHIURA Habitat 1. Adult worms in caecum of man, also in appendix and colon. 2. Eggs in faeces. Morphology 1. Body resembles a whip with hair
like anterior 3/5 part and much stouter posterior 2/5 part. 5. Eggs brown,
barrel-shaped with a plug at each pole; 50 µ x 25 µ; contain
a fertilized unsegmented ovum. - I II 'I
.
Chart : Life cycle of Trichuris trichiura Pathogenicity Generally symptomless; occasionally produces appendicitis. Chemotherapy As in Enterobius vennicularis.
TRICHINELLA SPIRALIS Habitat 1. Adult worms in small intestine of rat, pig, and man. 2. Larvae liberated in blood stream, encyst in muscles. 3.
Infected larvae encysted in flesh of pig and man. Morphology (a) Male worm (rarely
found)
(b)
Female worm Life Cycle
Chart : Life cycle of Trichinella spiralis Pathogenicity 1. Nausea, vomiting,
colic, diarrhoea; occasionally haemorrhage. Chemotherapy Thiabendazole (Mintezol) L5 g after evening meal to be repeated after next morning meal, ANKYLOSTOMA DUODENALE Habitat 1. Adult worms in
jejunum, occasionally in duodenum of man. Morphology (a) In both sexes
4. Mouth cavity
(buccal capsule) large and conspicuous; lined with chitin. 7. Oesophagus, opens
at the base of mouth cavity.
(b) Male worm: 1. 1 cm long, 0.5 mm
broad. (c) Female worm 1. 1.2 cm long, 0.6
mm broad. 3. Female genitalia consist of two long coiled tubes which unite to form a common vagina which opens at vulva. 4. The distal part of each duct is ovary, middle part the oviduct and the terminal part, the uterus. (d) Eggs.
Chart : Life cycle of Ankylostoma duodenale Pathogenicity 1. Grounds itch and urticaria. 2.
Anaemia.
Diagnosis Ova in faeces Chemotherapy WUCHERERIA BANCROFTI Habitat Adult worms in lymph
glands, lymphatic vessels, superficial abscesses, retroperitoneal tissue and
other sites. Morphology 3.
Anterior end is
rounded and bulging.
Chart : Life cycle of Wuchereria bancrofti Pathogenicity Filariasis characterised
by: 5. Elephantiasis of legs, scrotum and vulva 6. Chyluria. Chemotherapy Diethylcarbamazine citrate (Hetrazan) 50-100 mg thrice a day for 3-4 weeks. Diagnosis Microfilariae in night blood smear. LOA LOA Habitat 1. Adult worms in
subcutaneous connective tissue, mesentery, and parietal peritoneum; more
rapidly in the body and can be seen in subconjunctival
tissue of the eye. Morphology 1. Adult male
measures 3 cm in length 3.35 min in breadth; adult female measures 6 cm in length, 0.45 mm
in breadth. 3. Microfilariae sheathed with irregular outline, 250µ x 8µ; with nuclei extending to the tip.
Same as in Wuchereria bancrofti with only a different insect host. Pathogenicity Calabar swellings on
various parts of body. Microfilariae in mid-day smears. Chemotherapy As in W. bancrofti. DRACUNCULUS MEDINENSIS Habitat 1. Adult females in subcutaneous tissue, chiefly of legs, ankle and feet, and in intermuscular connective tissues. 2. Where about of male worms not known (In fact it has been detected in few historic cases only). 3. Microfilariae found on ulcerated surface in the centre of which the prolapsed uterus of female worm is often visible. 4. Developmental forms of infective larvae occur in the body of cyclops. Morphology 1. Adult female measures 120 cm in length and L5 mm in breadth; adult male measures 2 cm in length. 2. Head has chitinous shield. 3. Vulva is just behind the head. 4. Larvae with long, tapering tail, 500 µ x 20 µ Life Cycle
Chart : Life cycle of Dracunculus medinensis Pathogenicity Skin ulcers and inflammation. Diagnosis Larvae in washings of ulcer. Chemotherapy As in W. bancrofti. GENERAL Parasites Spread by Water A. Protozoa B. Helminths (a) Cestodes (b) Trematodes
(c) Nematodes I. Ascaris lumbaricoides
4. Ankylostoma duodenale
Orthropod Borne Parasites :- A. Protozoa B. Helminths (b) Trematode: [c] Nematodes 1. Ascaris lumbaricoides 2. Trichuris trichiura 3. Strongyloides stercoralis 4. Ankylostoma duodenale 5. Nectar americanas 6. Wuchereria bancrofti 7. Loa loa 8. Dipetalonema 9. Onchocera volvulus 10. Filaria ozzardi 11. Dracunculus medinensis Parasites Found on Skin :- (1) Spirochaeta pallida
Parasites Found in Muscle :- (1) Leishmania forms in Trypanosoma cruzi [2] Sarcocystis [3] Cysticercus cellulosae [4] Trichinella spiralis – encysted larvae
Parasites found in Intestines :- Taenia solium Taenia saginata Hymenolepsis nana Dibothriocephalus latus Fasciolopsis buski Heterophyes heterophyes Ascaris lumbaricoides Enterobius vermicularis Ankylostoma duodenale Nectar americanas Trichinella spiralis
Parasites found in Intestinal wall (1) Entamoeba
histolytica - unencysted form Parasites found in Liver (6) Hydatid cysts
Parasites found In Spleen (1) Malaria pigment (2) Leishmania (3) Cystcercus cellulosae (4) Hydatid cysts (5) Eggs of Schistosoma haematobium (6) Eggs of Schistosoma mansoni.
Parasites found in Lungs (1) Cysticerus cellulosae
Parasites found In Blood (1) Spifillum minus (2) Plasmodium majaliae (3) Plasmodium vivax (4) Plasmodium falcipaium (5) Plasmodium ovale (6) Trypanosoma gambiense (7) Trypanosoma donovani (rare) (8) Leishmania cruzi (9) Larvae of Wuchereyia bancrofti (10) Microfilaria malayi (11) Larvae of Loa loa (12) Larvae of Dipetalonemaperstans (13) Larvae of "Filaria" ozzagdi. |



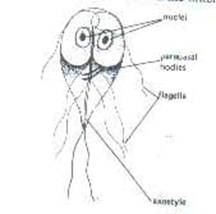













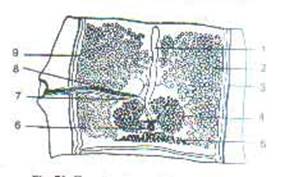

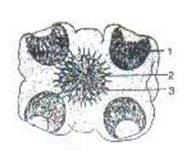


















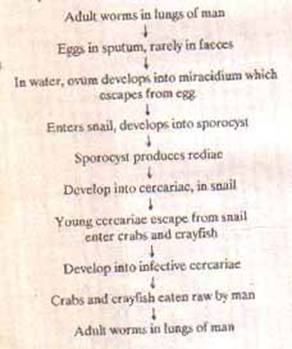



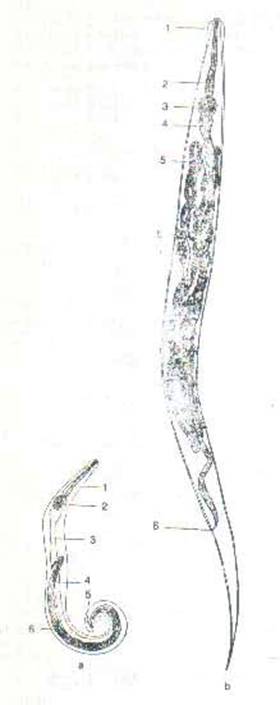













|
Paperback and Kindle Links at ukmall.net Publish On Amazon Free by Dr K Chaudhry |
|
|
ITI : Fitter Mnemonics by Dr K Chaudhry |
|
|
Tally ERP 9 Made Easy by Dr K Chaudhry |
|
|
Free Localhost : Make Your Computer A php Machine by Dr K Chaudhry |
|
|
Publish On Createspace Free by Dr K Chaudhry |
|
|
Anatomy Mnemonics by Dr K Chaudhry |
|
|
Physiology Mnemonics by Dr K Chaudhry |
|
|
Biochemistry Mnemonics by Dr K Chaudhry |
|
|
Pathology Mnemonics by Dr K Chaudhry |
|
|
Pharmacology Mnemonics by Dr K Chaudhry |
|
|
Forensic medicine Mnemonics by Dr K Chaudhry |
|
|
Medicine Mnemonics by Dr K Chaudhry |
|
|
Surgery Mnemonics by Dr K Chaudhry |
|
|
Obstetrics & Gynaecology Mnemonics by Dr K Chaudhry |
|
|
Ophthalmology Mnemonics by Dr K Chaudhry |
|
|
Medicine Made Easy by Dr K Chaudhry |
|
|
Patho Micro Made Easy by Dr K Chaudhry |
|
|
Medical Laboratory Techniques by Dr K Chaudhry |
|
|
MCQuestions in Paraclinical Sciences by Dr K Chaudhry |
|
|
Mere Geet, Meri Awaaz, Meri Sanvednaayen by Dr K Chaudhry |
|
|
Astrology Made Easy by Dr K Chaudhry |
|
|
Affiliate Marketing Tips & Scripts by Dr K Chaudhry Global Book Shop Online B-1/104 Paschim Vihar, New Delhi 110063 Tel: 01142316457, 9810570740, 9810571993 ukmall.net facebook.com/doctorkc youtube.com/drksongs |
|